Download
1 / 29
310 likes | 477 Vues
The Connection between Mental Health and HIV/AIDS: Implications for Clinical Care and Research. Robert H . Remien , Ph.D. Milton L. Wainberg , M.D. Katherine S. Elkington, Ph.D. HIV Center for Clinical and Behavioral Studies, Columbia University and NYSPI. Overview.

E N D
The Connection between Mental Health and HIV/AIDS: Implicationsfor Clinical Care and Research Robert H. Remien, Ph.D. Milton L. Wainberg, M.D. Katherine S. Elkington, Ph.D. HIV Center for Clinical and Behavioral Studies, Columbia University and NYSPI
Overview • The Intersection of mental health, substance abuse and HIV/AIDS • Deployment-focused intervention development: • Three research examples
The Intersection of Mental Health, Substance Use and HIV/AIDS
Mental illness and HIV Risk Behaviors • Specific Diagnoses: Inconsistently associated with risk • Symptoms: • Positive psychotic sx cluster multiple partners; IDU • excitement sx sexual activity; sex exchange; condom use • Depressed/anxious sx STDs; poor condom negotiation skills; multiple partners; inconsistent condom use • High rates of co morbid substance use • High rates of childhood abuse • Problematic current interpersonal relationships • Poverty / low SES : sex exchange • Stigma and Discrimination (Meade & Sikkema, 2005, 2006; Donenberg & Pao, 2005)
Substance Use and HIV Risk Behaviors Substance use and disorder linked to HIV/STI risk behaviors Type of substance: alcohol, stimulants, club drugs Amount and frequency of use: Addiction – sex exchange Motivation for use (social anxiety; expectancy theory) Role of environmental factors: peers, family Method of data collection Cross-sectional, longitudinal, event-level analysis (daily diary studies) 5
Mental Health and Substance Use Problems Among Subpopulations at High Risk for HIV IDU: ↑ rates of SUD and other psychiatric disorders MSM: ↑ rates of SUD and depression SW: ↑ rates of childhood sexual abuse, SUD, and PTSD Criminal/Juvenile justice: ↑ childhood sexual abuse; SUD and psychiatric disorders (particularly PTSD) All groups: Stigma; legal sanctions; poor access to services; high risk interpersonal relationships — all associated with ↑ risk behaviors
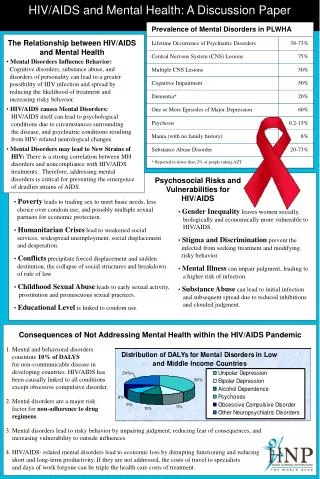
RAND HCSUS Study: 2,864 HIV+ Medical Patients Any Psychiatric Disorder: 48% Major depression 36% Dysthymia 27% Generalized anxiety disorder 16% Panic attack 11% Drug dependence 13% Problematic alcohol use 19% (Bing et al Arch. Gen. Psych. 2001) Psychiatric and Substance Use Disorders among PLWHA
Impact of Mental Health and Substance Use Problems for PLWHA Mental health and substance use problems can: • Impair the quality of one’s life • Interfere with HIV treatment adherence • Interfere with self-care behaviors and increase risk behaviors • Result in acting out verbally or physically • Impair ability to cope with daily events, including childcare • Increases morbidity and mortality
IPV Child abuse Stigma Interpersonal Strained/poor family & peer relationships Marginalized /risky peer groups Alcohol myopia “Social lubricant” (self medication) Acute intoxication (e.g. impaired judgement) Symptoms (e.g. paranoia, anxiety, depression, psychosis) Addiction Mental Illness Substance Ab/use HIV RISK BEHAVIORS Non Adherence to treatment and Care Environmental/ Structural Poor housing Transportation/ access to health care Stigma Neighborhood Disintegration Poverty
Deployment-Focused Intervention Development Implications for Intervention, Treatment, and Care
HIV Prevention with Psychiatric Patients in Brazil: Planning a National Response Milton L. Wainberg, MD Associate Clinical Professor of Psychiatry, Columbia University PRISSMA Project / NIMH R01-65163/ 2002-2006
Background • Worldwide, adults with severe mental illness (SMI) have elevated rates of HIV infection (between 0.8% and 23.8%)relative to the general population (3 to 5 times) • Few (n=7; 919 participants) HIV prevention interventions have been tested for efficacy – all of them in the US (Kalichman 1995, Kelly 1997, Susser 1998, Weinhardt 1998, Otto-Salaj 2001, Carey 2004, Berkman 2006) • There is no single “gold standard” HIV prevention intervention for the SMI PRISSMA Project / NIMH R01-65163/ 2002-2006 & 2006-2011
Summary of HIV PreventionResearch among SMI - 2001 PRISSMA Project / NIMH R01-65163/ 2002-2006 & 2006-2011
PRISSMA I Model AIDS and Behavior, 2007 • Optimizing Fidelity: • HIV Prevention Principles 2) Optimizing Fit: Adaptation Principles 3) Balancing Fidelity and Fit: Intervention Adaptation 4)Pilot Testing and Refining: Final Intervention PRISSMA Project / NIMH R01-65163/ 2002-2006 & 2006-2011
RCT Study Design Screen Baseline assessment* Orientation HIV – 8 sessions Health – 8 sessions Post-intervention assessment** 3- & 6-months follow-up assessments* HIV – 3 boosters Health – 3 boosters Post -booster assessment** 12-months follow-up assessment* PRISSMA Project / NIMH R01-65163/ 2002-2006 & 2006-2011 * Diagnoses, risk behaviors, mediators/moderators ** Process measures, mediators/moderators
Recruitment Recruitment ended 7 months early!!!!!!
Summary of HIV PreventionResearch among SMI – 2011/2014 PRISSMA Project / NIMH R01-65163/ 2002-2006 & 2006-2011
Working with systems from the beginning: A Case example with JJS youth K01MH089832 ; PI: Elkington
What’s Unique about JJS Youth? • Juvenile detainees are at high risk for HIV/STIs: • Higher rates of HIV/STI risk behaviors • Higher rates of substance use and mental health (MH) disorders • Numerous contextual factors that increase risk • Peers, families, neighborhoods
Intervening with Just the Youth….…is that Enough? • Need to involve other domains or systems of risk and protection • Systems may act directly (e.g. family, peer group) or may be more distal (neighborhood, JJS) • Family is key to promoting or off-setting risk • GOAL: Target HIV/STI risk by addressing MH and SU problems and improving family functioning within context of the JJS
MACROSYSTEM Social-Cultural Context Immigration Policy • Exosystem • Parents’ social support • Parents’ stress Language Poverty • Family MICROSYSTEM • Family functioning (conflict/support) • Caregiver monitoring/supervision • Caregiver discipline • Caregiver-youth communication • Caregiver-youth relationship satisfaction Cultural Family-School Mesosytem Parental monitoring homework Family-Peer Mesosytem Parental monitoring of peer activities • Youth • Substance use • Mental Health • HIV/STI knowledge • Safer sex and drug use • attitudes • Safer sex self-efficacy • Perceived HIV risk • Safer sex behavior • skills School Microsystem School Bonding Academic Achievement Peer Microsystem Perceived peer HIV/STI behavior Perceived peer HIV/STI norms HIV/STI sexual risk behavior Modified Ecodevelopmental Model Szapocznik & Coatsworth, 1999)
Developing the intervention • To develop and implement effective interventions that are targeted and sustainable: • Achieve buy in from treatment system and key-stakeholders involved • Probation, staff, families, youth • Formative work • Understand logistic and institutional-cultural contextual factors of the probation center and staff • Understand context of sexual risk for JJS youth including the role of the family
MACROSYSTEM Social-Cultural Context Immigration Policy • Exosystem • Parents’ social support • Parents’ stress Language Poverty • Family MICROSYSTEM • Family functioning (conflict/support) • Caregiver monitoring/supervision • Caregiver discipline • Caregiver-youth communication • Caregiver-youth relationship satisfaction Cultural JJS Family-School Mesosytem Parental monitoring homework Family-Peer Mesosytem Parental monitoring of peer activities • Youth • Substance use • Mental Health • HIV/STI knowledge • Safer sex and drug use • attitudes • Safer sex self-efficacy • Perceived HIV risk • Safer sex behavior • skills School Microsystem School Bonding Academic Achievement Peer Microsystem Perceived peer HIV/STI behavior Perceived peer HIV/STI norms HIV/STI sexual risk behavior Modified Ecodevelopmental Model 24
Phase 1 – Formative phase • Interview probation staff (n=12) • What is their perception of youth HIV/STI risk? • What is role of probation department in providing HIV/STI programming? • How would an intervention fit into current programming….. climate…… culture?
All staff perceived their youth to be at considerable risk for HIV/STIs and needed intervention program: • Sexually active at young ages; ↑ pregnancies • Impulsive; MH and SA abuse problems • Limited supervision and problematic role models (peers and family) • Implications for intervention development and delivery: • Great – we are on the right track, sexual risk is a problem • Addressing MH issues and SA is key • Staff think this is important to address • Staff recommend program to families and talk up program to get resistant families involved
Providers struggled to reconcile their role as POs with their responsibility of providing youth with services • “It’s not on the form so we don’t ask” • Address presenting problem rather than provide prevention for a potential problem • Social work vs. law enforcement: Differing views held by staff • Sex risk, HIV/STI rarely bought up - believe youth will not talk • Staff do not feel adequately trained to address sexual risk but would if they were trained • Implications for intervention development: • Add a sex risk screening question to intake assessment? • Alter culture: promote prevention for non-probation related issues • Task shifting: train subset of POs in youth sexuality and sexual risk reduction to deliver intervention
How would an intervention fit into current programming….. climate…… culture? • POs currently co-lead groups onsite at the probation department • On-site vs. off-site programming: Both services are available. • POs busy schedule: is there time to add additional programs • Family engagement always tricky • Implications for intervention development: • Build intervention into existing services and bundle • Work with community providers • Build in participation in HIV program as mandatory part of their probation
Developing the intervention cont’d • Develop a family-based intervention building on an existing efficacious youth-only intervention designed for youth on probation • 1st work group : youth and caregivers • Review interview data and existing interventions; role play and suggest changes • 2nd work group: probation staff • Work together to create actual intervention sessions drawing from other family-based interventions • Pilot test the intervention in department of probation • Deliver as part of co-located services offered • Work with CBOs to deliver to JJS families