Download
1 / 1
10 likes | 142 Vues
From Bad to Worse: Comorbidities and Chronic Lower Back Pain. Margaret Cecere JD, Richard Young MD, Sandra Burge PhD The University of Texas Health Science Center at San Antonio John Peter Smith Family Medicine Residency Program, Fort Worth. Introduction. Methods.

E N D
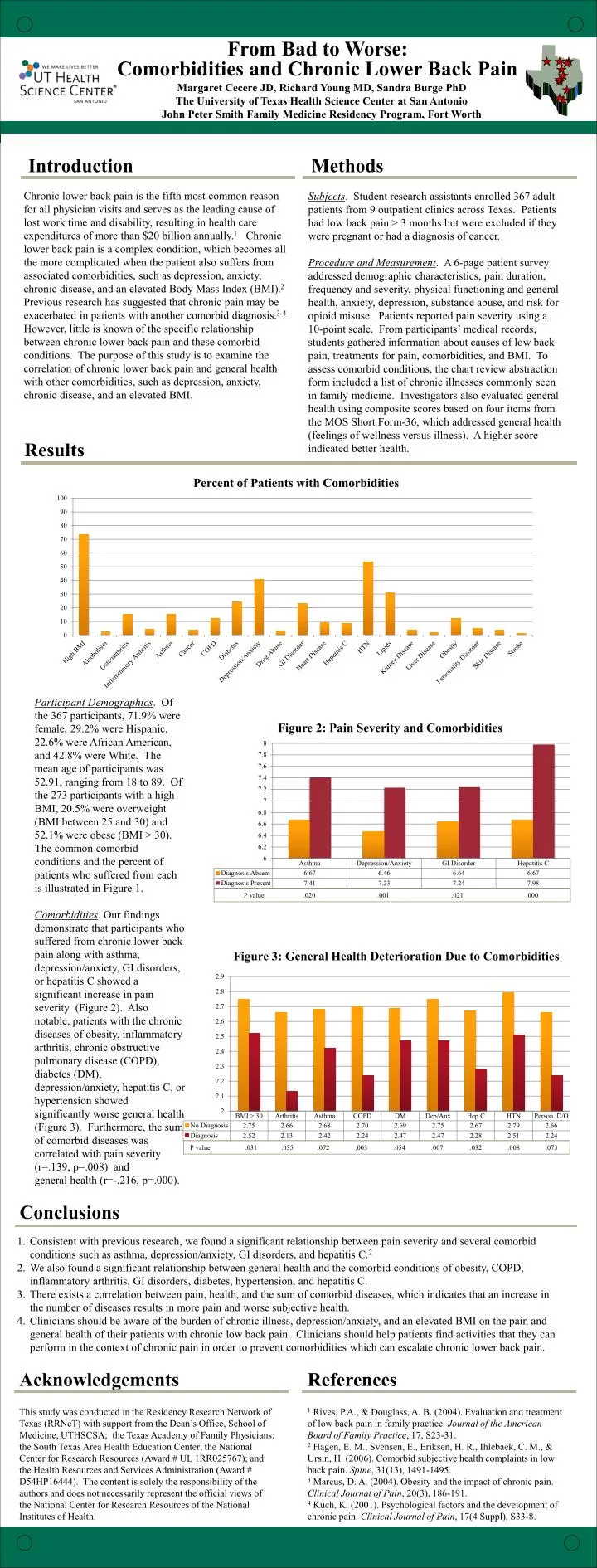
From Bad to Worse: Comorbidities and Chronic Lower Back Pain Margaret Cecere JD, Richard Young MD, Sandra Burge PhD The University of Texas Health Science Center at San Antonio John Peter Smith Family Medicine Residency Program, Fort Worth Introduction Methods Subjects. Student research assistants enrolled 367 adult patients from 9 outpatient clinics across Texas. Patients had low back pain > 3 months but were excluded if they were pregnant or had a diagnosis of cancer. Procedure and Measurement. A 6-page patient survey addressed demographic characteristics, pain duration, frequency and severity, physical functioning and general health, anxiety, depression, substance abuse, and risk for opioid misuse. Patients reported pain severity using a 10-point scale. From participants’ medical records, students gathered information about causes of low back pain, treatments for pain, comorbidities, and BMI. To assess comorbid conditions, the chart review abstraction form included a list of chronic illnesses commonly seen in family medicine. Investigators also evaluated general health using composite scores based on four items from the MOS Short Form-36, which addressed general health (feelings of wellness versus illness). A higher score indicated better health. Chronic lower back pain is the fifth most common reason for all physician visits and serves as the leading cause of lost work time and disability, resulting in health care expenditures of more than $20 billion annually.1 Chronic lower back pain is a complex condition, which becomes all the more complicated when the patient also suffers from associated comorbidities, such as depression, anxiety, chronic disease, and an elevated Body Mass Index (BMI).2 Previous research has suggested that chronic pain may be exacerbated in patients with another comorbid diagnosis.3-4 However, little is known of the specific relationship between chronic lower back pain and these comorbid conditions. The purpose of this study is to examine the correlation of chronic lower back pain and general health with other comorbidities, such as depression, anxiety, chronic disease, and an elevated BMI. Results • P value .020 .001 .021 .000 Participant Demographics. Of the 367 participants, 71.9% were female, 29.2% were Hispanic, 22.6% were African American, and 42.8% were White. The mean age of participants was 52.91, ranging from 18 to 89. Of the 273 participants with a high BMI, 20.5% were overweight (BMI between 25 and 30) and 52.1% were obese (BMI > 30). The common comorbid conditions and the percent of patients who suffered from each is illustrated in Figure 1. Comorbidities. Our findings demonstrate that participants who suffered from chronic lower back pain along with asthma, depression/anxiety, GI disorders, or hepatitis C showed a significant increase in pain severity (Figure 2). Also notable, patients with the chronic diseases of obesity, inflammatory arthritis, chronic obstructive pulmonary disease (COPD), diabetes (DM), depression/anxiety, hepatitis C, or hypertension showed significantly worse general health (Figure 3). Furthermore, the sum of comorbid diseases was correlated with pain severity (r=.139, p=.008) and general health (r=-.216, p=.000). Conclusions Consistent with previous research, we found a significant relationship between pain severity and several comorbid conditions such as asthma, depression/anxiety, GI disorders, and hepatitis C.2 We also found a significant relationship between general health and the comorbid conditions of obesity, COPD, inflammatory arthritis, GI disorders, diabetes, hypertension, and hepatitis C. There exists a correlation between pain, health, and the sum of comorbid diseases, which indicates that an increase in the number of diseases results in more pain and worse subjective health. Clinicians should be aware of the burden of chronic illness, depression/anxiety, and an elevated BMI on the pain and general health of their patients with chronic low back pain. Clinicians should help patients find activities that they can perform in the context of chronic pain in order to prevent comorbidities which can escalate chronic lower back pain. P value .031 .035 .072 .003 .054 .007 .032 .008 .073 References Acknowledgements 1 Rives, P.A., & Douglass, A. B. (2004). Evaluation and treatment of low back pain in family practice. Journal of the American Board of Family Practice, 17, S23-31. 2 Hagen, E. M., Svensen, E., Eriksen, H. R., Ihlebaek, C. M., & Ursin, H. (2006). Comorbid subjective health complaints in low back pain. Spine, 31(13), 1491-1495. 3 Marcus, D. A. (2004). Obesity and the impact of chronic pain. Clinical Journal of Pain, 20(3), 186-191. 4 Kuch, K. (2001). Psychological factors and the development of chronic pain. Clinical Journal of Pain, 17(4 Suppl), S33-8. This study was conducted in the Residency Research Network of Texas (RRNeT) with support from the Dean’s Office, School of Medicine, UTHSCSA; the Texas Academy of Family Physicians; the South Texas Area Health Education Center; the National Center for Research Resources (Award # UL 1RR025767); and the Health Resources and Services Administration (Award # D54HP16444). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources of the National Institutes of Health.