Atherosclerosis
Atherosclerosis. D S O’Briain April 2007. Atherosclerosis. Arteriosclerosis (hardening of the arteries) 3 types: Atherosclerosis (athero=porridge) plaques of lipid and fibrous tissue in vessel wall Less important forms of arteriosclerosis 2. Medial calcification (Monckeberg)

Atherosclerosis
E N D
Presentation Transcript
Atherosclerosis D S O’Briain April 2007
Atherosclerosis Arteriosclerosis (hardening of the arteries) 3 types: • Atherosclerosis (athero=porridge) plaques of lipid and fibrous tissue in vessel wall Less important forms of arteriosclerosis 2. Medial calcification (Monckeberg) 3. Small vessel (arteriolosclerosis) hyaline or hyperplastic
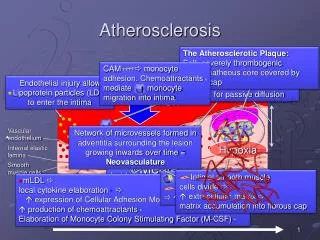
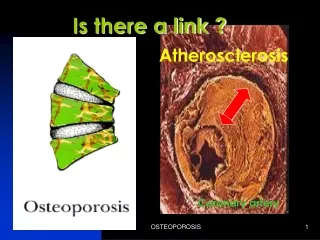
Atheromatous Plaque, Macroscopic • Distribution: Abdominal aorta> coronary > popliteal > descending thoracic >internal carotid > circle of Willis. • Spared: upper extremities, renal, mesenteric (except ostia). • Fibrous cap (white), deeper portion (grumous, yellow). • 3 - 15 mm diameter, raised, coalesce. • Scanty to numerous
Atheromatous Plaque Histology • Fibrous cap: Smooth muscle, WBC, connective tissue, collagen, elastic, proteoglycan. • Core: lipid debris, cholesterol, cholesterol esters, foam cells ( smooth muscle and macrophage), fibrin, plasma proteins, T-cells. • Periphery: neovascularisation, chronic inflammation.
Effects of Atheromatous Plaque Different effects in narrow (coronary) and wide (aorta) vessels Clinically silent Most plaques have no effect. Calcification: Identify on imaging. Complicated plaques Fissure Ulcerate: atheroemboli. Thrombose: occlude, embolise Haemorrhage: occlude. Consequences Stenose: Ischaemia, atrophy. Occlude (by thrombus or haemorrhage): Infarct. Aneurysm: pressure effects, leak (rupture)
Fatty streak Possible precursor of atheroma. • Spot (1mm), Streak (1x10mm). • Composition: Macrophages filled with lipid (foam cells) later smooth muscle cells with lipid droplets, extracellular lipid, T-lymphocytes, proteoglycans, collagen, elastin. • Incidence: More frequent with high milk/fat diet: • 10% first decade, 30% third decade, • May recede, persist or convert to fibrous plaque • Distribution: Aorta - unlike atheroma, Coronary arteries - like atheroma.
Intimal Cushion • White areas of diffuse intimal thickening composed of intimal smooth muscle and matrix (little collagen, no lipid), gelatinous lesion. • Degenerate effect of blood pressure and time. • But occur at ostia (atheroma sites).
Monckeberg’s Calcific Medial Sclerosis • Calcification of medium or small arteries • Both sexes, over 50 • Arteries: Femoral, radial, ulnar, genital. • Cause: vasotonic factors, adrenaline, nicotine. • Effect: none, visible in imaging
Arteriolosclerosis • Hyaline change in vessel walls. • Pathogenesis - plasma leakage, smooth muscle matrix. • Associations - hypertension, diabetes, age. • Benign - hyaline narrowing. • Hyperplastic - onion skin (fibrinoid necrosis). • Sites: Kidney, gall bladder, intestine, periadrenal, pancreatic.
Theories of Atherogenesis • Virchow - imbibation • (lipid theories) • Rokitansky - encrustation • (thrombotic theories)
Atherosclerosis Risk Factors Hyperlipidemia. LDL (low density lipoprotein) Hypertension: 160/95 Vs 140/90,- Risk X 5. Increases: Atheroma, IHD, CVD. Risk decreases with therapy. Cigarettes: More AS, more sudden death, Risk increased by 70-200%. Decreases after cessation. Diabetes: More AS, MI x 2, Increased CVD, PVD risk increased x 8-150. Other: Physical activity, stress, obesity, oral contraceptives, hyperuricemia, high carbohydrate intake, male, age, family history, homocystinemia. Multiple Factors: More than additive. NOTE: IHD ischaemic heart disease, CVD cerebrovascular disease, PVD peripheral vascular disease AS atherosclerosis, MI myocardial infarction,
Role of lipid in Atherosclerosis 1. Found in plaque 2. Experimentally raised lipid -> AS 3. Hyperlipidemias -> AS 4. Populations with high lipids -> high AS rate 5. Treat hyperlipidemia - decrease AS.
Risk of Atherosclerosis • High: Raised LDL (70% cholesterol), triglyceride and VLDL. • Low: Raised HDL. • Risk increases with increased cholesterol level (risk x 5 with cholesterol increase 220 to 265) • Increased intake cholesterol and triglycerides - increases serum cholesterol. • Omega 3 fatty acids (fish) protective
How Hyperlipidemia may damage intima More serum LDL, more cellular penetration. • LDL with proteoglycan - avid uptake. • LDL modified - lysosomal uptake. • LDL - directly damages endothelial cell. • Oxidised lipoproteins: Endothelial injury, smooth muscle injury, foam cells - scavenger receptor, chemotactic.
Intimal dysfunction • Cause: Mechanical, Haemodynamic stress, Immune complex, Radiation, Chemotherapy. • Association: Hypertension, Stress, Cigarettes. • Effect: Increased intimal permeability, adhesion, smooth muscle proliferation, atheroma (if hyperlipidemia )
Macrophage • Family: Monocyte, histiocyte, macrophage, epithelioid cell, giant cell, granuloma • Monocytes adhere, migrate, phagocytose • Have scavenger receptor - modified VLDL receptor (Lipid internalised, hydrolysed, esterified -> lipid droplet). • Monocytes produce: IL-1, TNF (increased adhesion), chemotaxis factors, toxic O2, PDGF, TGF beta -> smooth muscle
Smooth muscle proliferation • Origin: From media (or myointima) • Stimulus: PDGF (from platelets, macrophages, endothelial and smooth muscle cells), FGF, EGF, TGF. • Inhibit: Heparin, TGF-B. • Result: Smooth muscle cells produce extracellular matrix and foam cells (atheroma)
Arterial Injury Permeability increases. Adhesion of platelets, monocytes Factors released Smooth muscle migrates to intima, proliferates and produces extracellular matrix, collagen, elastin, proteoglycans Monocytes - phagocytose Lipid deposited
Other Theories of Atherogenesis • Primary smooth muscle proliferation: monoclonal growth (as a form of leiomyoma) • Cause: Exogenous (hydrocarbon, virus), endogenous (cholesterol) • Experimentally: Plaques in Marek chicken virus, anthracycline, herpes mRNA in plaque
Ischaemic Heart Disease Epidemic • Causes 80% of cardiac mortality • Peaked in US in 1960s, 40% decline since • Different patterns in some Western countries • Cause of decline: Changing lifestyle (diet, smoking, exercise) • Better therapy (CCU, thrombolysis, arrhythmia therapy, CABG, angioplasty)
Atherosclerotic Coronary Artery Disease: Clinical Syndromes • Silent Infarct • Angina Pectoris • Myocardial Infarct • Chronic Ischaemic Heart Disease • Sudden Death
Atherosclerotic Coronary Artery Disease: Clinical Syndromes • Silent Infarct • Angina Pectoris • Myocardial Infarct • Chronic Ischaemic Heart Disease • Sudden Death
Aneurysms • Localised abnormal dilation of vessel. • Types: Saccular, fusiform, cylindroid, dissection. • Complications: Pressure, thrombus, rupture. • Aetiology: Atherosclerosis, cystic medial necrosis, syphilis, trauma (arteriovenous aneurysm), PAN, infections, (mycotic), congenital (berry).
Atherosclerotic Aneurysm • Males of 50+, frequently (50%) hypertensive • Abdominal aorta (between renal artery and aortic biforcation). (Thoracic aorta, renal, mesenteric arteries) • Complications; • Rupture (if >6 cm, 50% rupture in 10 years) • surgical mortality 50% (unruptured 5%) • Compression - ureter, vertebrae • Occlusion (thrombus, pressure) • Embolism • Abdominal mass
AtherosclerosisPeripheral vascular disease • Pain (claudication) • Ischaemic changes • Gangrene • General atheroma risk factors • But 100 times more frequent in diabetes
AtherosclerosisMesenteric ischaemia • Coeliac, superior mesenteric artery) • Aymptomatic • Intestinal angina (pain after food) • Intestinal ischaemia • Bloody diarrhoea • Infarction/gangrene • obstruction
AthersclerosisCerebrovascular disease • Thrombosis (embolism, haemorrhage are other import factors in stroke) • Sites of thrombotic occlusion:carotid bifurcation, middle cerebral and basilar arteries) • Transient ischaemic attack (TIA), cerebrovascular accident (CVA), (stroke)