Atherosclerosis
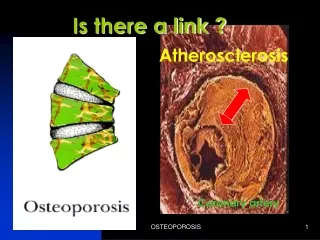
Atherosclerosis. Focal plaques within the intima containing cholesterol and cholesterol esters (CE) Affects large and medium sized arteries Causes coronary heart diseases (CHD) Hypercholesterolemia – high serum cholesterol level Elevated LDL and triglycerides –

Atherosclerosis
E N D
Presentation Transcript
Atherosclerosis • Focal plaques within the intima containing cholesterol and cholesterol esters (CE) • Affects large and medium sized arteries • Causes coronary heart diseases (CHD) • Hypercholesterolemia – high serum cholesterol level Elevated LDL and triglycerides – associated with increase risk Serum HDL levels – inversely related to risk
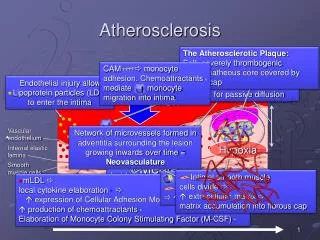
Pathogenesis • Chronic inflammatory response of the vascular wall to endothelial injury or dysfunction • Elevated plasma LDL levels causing the deposit of LDL in the subendothelium of blood vessels • Oxidation of transmigrated LDL • Activation of endothelial cells • Recruitment of monocytes/macrophages which ingest oxLDL through scavenger receptors • Formation of foam cells – fatty streaks • Proliferation of smooth muscle cells • Deposition of extracellular matrix proteins
lumen intima Monocyte Recruitment LDL
Formation of Atherosclerotic Plaques lumen neointima Lipid Core
Plaque Rupture and Thrombosis Tissue Factor Platelet Aggregation Lipid Core
Exogenous Pathway • Route of uptake of dietary lipids. • Chylomicrons (CM) – complexes of TG, CE and apoproteins • Chylomicron remnants – CM after removal of most TG • CM are degraded by lipoprotein lipase on endothelial cells of adipose tissue and muscle. After removal of TG for storage, CM remnants are transported to the liver. • Results: Dietary TG is stored in adipose tissue and muscle. Cholesterol is stored in liver or excreted into the bile as cholesterol or bile acid.
Endogenous Pathway • Route for distribution of CE from liver to target cells • VLDL – secreted by the liver to plasma and transported to adipose tissue and muscle where lipoprotein lipase extracted TG. The remnant IDL is either taken up by the liver or circulates until the remaining TG is removed, forming LDL particles which are rich in cholesterol. • LDL is cleared from plasma by LDL receptor-mediated endocytosis. • Results: 1) Transfer of TG from liver to target cells via VLDL; 2) Transfer of CE from liver to target cells via LDL; 3) Feedback regulation of cholesterol homeostasis by LDL receptor expression; 4) Creation of a steady state LDL-CE reserve in plasma.
Reverse Transport of Cholesterol • Route for cholesterol recovery • As cell dies and the cell membrane turnover, free cholesterol is released into the plasma. It is immediately absorbed onto HDL particles, esterified with a long chain fatty acid by lecithin:cholesterol acyltransferase (LCAT), and transferred to VLDL or IDL by a cholesteryl ester transfer protein (CETP) in plasma. Eventually, it is taken up by the liver as IDL or LDL. • Results: Recovery of cholesterol from cell membranes and reincorporation into LDL pool or return to liver.
De Novo Cholesterol Biosynthesis • Liver synthesizes 2/3 of cholesterol made by the body. The rate limiting enzyme is 3-hydroxyl 3-methyl glutaryl (HMG)-CoA reductase. • Results: Provide feedback regulation by cholesterol concentrations in cells.
Cholesterol Excretion by Enterohepatic Circulation • Bile salts are synthesized from cholesterol in the liver, released into the intestine and recycled. A small amount of bile acid is excreted. • Results: Conversion of liver cholesterol to bile salts for excretion.
Genetic Defects of Lipid Metabolism • Monogenic Familial hypercholesterolemia (homozygous or heterozygous) defect: inactive LDL receptor Familial lipoprotein lipase deficiency defect: inactive lipoprotein lipase Familial combined hyperlipidemia defect: unknown • Polygenic/multifactorial – commonly encountered Hypercholesterolemia Hypertriglyceridemia
Therapeutic Strategy • Identify patients at risk 1. Routine screening of serum cholesterol 2. Assessment of contributing risk factors • Non-pharmacologic therapy 1. Diet modification 2. Lifestyle modification C. Pharmacologic therapy
Lovastatin aka “statins”(HMG-CoA reductase inhibitors) • Action: competitively inhibits HMG-CoA reductase, the key enzyme for de novo cholesterol biosynthesis. • Results: 1) cells express more LDL receptors; 2) decreased serum LDL levels; 3) suppresses production of VLDL in liver; 4) increased HDL levels; 5) increased HDL/LDL ratio. • Advantages: specific; effective; well-tolerated. • Disadvantages: hepatotoxicity; myopathy; most expensive; contradicted in pregnant and nursing women.
Bile acid sequestrants(colestipol, cholestyramine, colesevelam) • Taken orally, not absorbed from the intestine. • Action: Anion exchange resins which bind negatively charged bile acids in the small intestine. • Results: 1) increased conversion of cholesterol to bile acid in hepatocytes; 2) increased synthesis of cholesterol and LDL receptors in hepatocytes; 3) decreased serum LDL and cholesterol levels. • Advantages: clinically safe; effective. • Disadvantages: unpleasant GI effects; interference with GI drug absorption (e.g., coumarin); may exacerbate hypertriglyceridemia (unknown mechanism).
Ezetimibe • Action: inhibits dietary cholesterol uptake by jejunal enterocytes by binding to a key mediator of cholesterol absorption – Neimann-Pick C1-Like1 (NPC1L1). • Results: 1) reduction of cholesterol incorporation into chylomicrons and delivery to hepatocytes; 2) increased synthesis of cholesterol and LDL receptors in hepatocytes; 3) decreased serum LDL and cholesterol levels. • Advantages: clinically safe; effective; used as monotherapy in statin-intolerant patients; also used in combination with statins in statin-tolerant patients for further reduction of serum LDL and cholesterol. • Disadvantages: no effect on TG absorption; a new class of anti-atherosclerotic drug – long term effect not known.
Niacin (nicotinic acid) • Action: Acts through a Gi-coupled GPCR to decrease cAMP levels. Inhibits hormone-sensitive lipase involved in lipolysis in adipose tissue and decreases free fatty acid (FFA) transfer to the liver for synthesis of triglycerides. • Results: 1) decreased production and release of VLDL by liver; 2) decreased serum levels of VLDL as well as LDL and TG; 3) reduced clearance of HDL or increased serum level of HDL; 4) increased HDL/LDL ratio. • Advantages: long clinical experience; effective; least expensive. • Disadvantages: evokes flushing, itchiness, dyspepsia and GI discomfort, contraindicated for diabetic patients and pregnant women; adverse effects in hepatic diseases and reactivation of gout.
Fibrates (prototype: clofibrateUS: gemfibrozil; Europe: fenofibrate) • Action: acts through peroxisome proliferator activated receptors (PPARs) to stimulate gene transcription of lipoprotein lipase; increases the clearance of VLDL and reduce plasma TG levels; decreases VLDL synthesis which also lower serum LDL levels; increases plasma HDL by increased synthesis and/or decreased clearance. • Results: decreased serum TG and cholesterol; increased HDL/LDL ratio. • Advantages: recent clinical data support safety and efficacy; well-tolerated, potential anti-thrombotic effect. • Disadvantages: more effective in reducing TG than cholesterol; contraindicated in patients with renal failure. Clofibrate has restricted usage because of toxicity.
CETP Inhibitors (Torcetrapib) • Action: Inhibits the transfer of cholesterol ester from HDL to VLDL. • Results: 1) increased serum level of HDL; 2) by itself, no effect on LDL levels; 3) use in combination of statins to lower LDL with further increase in HDL.
Combined Drug Therapy • Advantages: Synergistic approaches utilizes complementary mechanisms of drug actions; reduces effective doses of single drug to prevent side effects. • Hypercholesterol without hypertriglycerides: Bile acid sequestrant plus lovastatin Ezetimibe plus lovastatin Bile acid sequestrant plus lovastatin plus ezetimibe Bile acid sequestrant plus nicotinic acid Bile acid sequestrant plus gemfibrozil (less common)
Hypercholesterol with hypertriglycerides: Nicotinic acid plus lovastatin Lovastatin plus gemfibrozil Nicotinic acid plus lovastatin plus bile acid sequestrant
Probucol(lipophilic antioxidant) • Action: Taken up by LDL particles and endothelial cells. Inhibits oxidation of LDL and prevents ingestion by macrophage foam cells. Decreases HDL production. • Results: 1) decreases atherosclerotic plaque formation; 2) small reduction in serum LDL-cholesterol; 3) greater reduction of serum HDL-cholesterol. • Advantages: may be used in combination therapy with other drugs that lower serum LDL-cholesterol. • Disadvantages: not effective in single drug therapy; no long term clinical data.