Download
1 / 71
750 likes | 1.27k Vues
Management of Chemo-immunotherapy toxicities. Characteristics of Cancer Cells –the problem to us all. Cell cycle acceleration with rapid division Immortality cell due to diminished apoptosis Altered cell-cell communication and disordered proliferation

E N D
Characteristics of Cancer Cells –the problem to us all • Cell cycle acceleration with rapid division • Immortality cell due to diminished apoptosis • Altered cell-cell communication and disordered proliferation • Invasiveness and metastasis threaten healthy organs and ultimately compromises the host
Cancer Cells versus the best of men – left unchecked -- who is likely to win?
Goal of Cancer Treatments • Curative • Palliative • Minimize toxicity • Improve quality of life • Scientifically garner lessons learned to improve future care
Established Treatment Modalities • Surgery • Radiotherapy • Chemotherapy including stem cell transplant • Endocrine therapy • Immunotherapy • Biological therapy
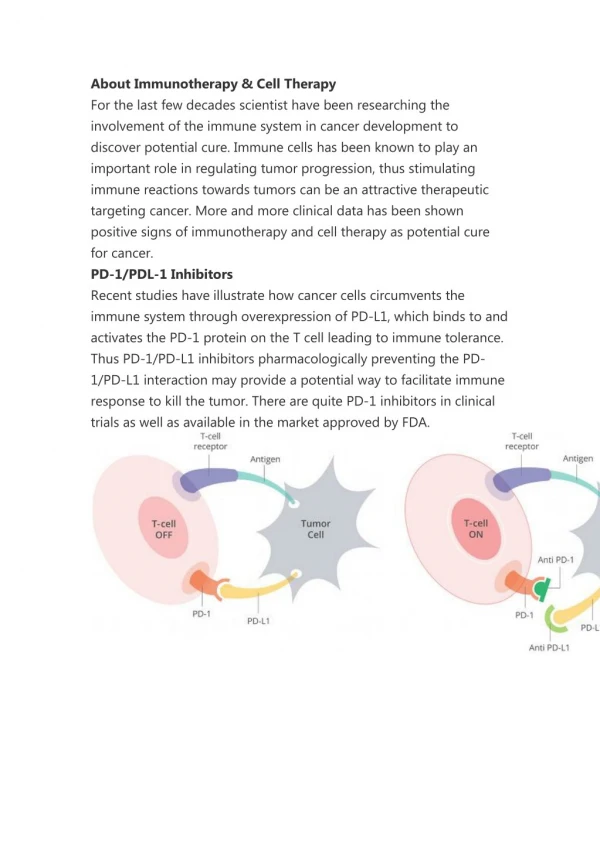
Chemo-immunotherapy Classes • Targeted therapies target moleculary defined target: Gleevec, gefitinib, sunitinib and bortezomib • Differentiating agents : retinoids, ATRA and bexarotene, arsenic trioxide • Hormone therapy in hormone driven cancers such as breast, prostate, and endometrial cancers • Immunotherapy can be active or passive or non-specific: rituximab, campath, IL-2, BCG, interferon • Immunomodulating drugs include thalidomide, lenalidomide, Provenge
Alkylating agents directly damage DNA and not phase-specific • Antimetabolites –interrupt DNA and RNA and are S- phase cell cycle specific. • Anti-tumor antibiotics such as anthracyclines interfere with DNA replication enzymes • Not phase specific • Topoisomerase inhibitors -- interfere with topoisomerases & copying of DNA strands • Mitotic inhibitors -- plant alkaloids and interfere with mitosis • Mostly M- phase of the cell cycle
CommonToxicities to many of these agents • Myelosuppression • Gastrointestinal – nausea/vomitting • Dermatology – Alopecia, hand-foot syndrome • Neurologic toxicity • Tumor lysis syndrome
Case • Staff Seargent Jones is a 25 y/o female with metastatic colorectal cancer in the setting of family history of HNPCC • She started cycle 2 chemoimmunotherapy with 5-FU and cetuximab 2 days ago • She now presents to you as ER admitting resident with c/o nausea/vomitting and inability to keep food down • Exam: • VS: Bp 95/50 HR 110 Temp 98.5 • ill-appearing but no focal findings except mild cachexia and hyperpigmented palms, feet and lips • Hgb 8, wbc 3.6, plt 40, ALT 100, AST 79, Tbili 1.3 Bun 35 sCR 1.8 • You will now do what?
Gastrointestinal Complication • TOXIC INJURY OF ORAL AND GASTROINTESTINAL MUCOSA • CLINICAL SYMPTOMS - stomatitis with ulceration and pain - abdominal pain, watery stools not related to infection, hemorrhagic stools • CONSEQUENCES - infections mainly with opportunistic endogenous GI microflora - bleeding - perforation - worsening of general status due to poor nutrition
NAUSEA AND VOMITING • PATOGENESIS • Not well understood • One hypthesis = chemotherapy causes 5HT release from enterochromafin cells of stomach and gut, activating its receptors and initiating depolarization of vagus nerve • Uncontrolled chemotherapy induced naseau/vomitting results in - difficulties with oral drugs administration and oral feeding - exacerbation of oral cavity, pharynx and esophagus mucosal injury - Suboptimal chemo treatment due to drug discontinuation
Scope of the problem -- Chemotherapy Induced Nausea Vomitting (CINV) • Incidence of acute and delayed N&V prospectively studied in 298 adult patients receiving HEC or MEC for the first time from 14 oncology practices in six countries • Patients completed a 6-day diary including emetic episodes, nausea assessment, and antiemetic medication use • Result: • Overall incidence of acute nausea > 35% and acute emesis = 13% • Delayed nausea with HEC pt = 60% and emesis = 50% • Delayed nausea with MEC pt = 52% and emesis = 28% • Delayed symptoms appeared without acute symptoms after HEC (emesis, 38%; nausea, 33%) and MEC (emesis, 19%; nausea, 21%) • ** >75% of physicians and nurses underestimated the incidence of delayed CINV after both HEC and MEC Grunberg SM, Deuson RR, Mavros P, et al.: Incidence of chemotherapy-induced nausea and emesis after modern antiemetics. Cancer 100 (10): 2261-8, 2004
Classification schema • Acute • Begins 1-2 hrs after initiation, peaks at 4 hrs • Delayed • >24 hours after chemo • Anticipatory/hyperacute • Prior to chemotherapy as a conditioned reaction to prior episodes of emesis with treatment
Patient-specific risk factors • Higher-risk groups • Young • Female • High pretreatment expectation of nausea • Poor n/v control with prior chemotherapy • High ETOH consumption = ? negative risk factor
#1 risk factor is drug dependent • The type of chemotherapy delivered • Dose • schedule of administration • route • individual patient variables
Chemo Emetogenic Potential • High (level 4) • >90% risk of emesis without treatment • Moderate (level 3) • 31-90% risk of emesis without treatment • Low (level 2) • 10-30% risk of emesis without treatment • Minimal (level 1) • <10% risk of emesis without treatment Kris MG, Hesketh PJ, Somerfield MR, et al.: American Society of Clinical Oncology guideline for antiemetics in oncology: update 2006. J Clin Oncol 24 (18): 2932-47, 2006
Classes & examples of Anti-emetics • 5-HT3 Receptor Antagonists: Ondansetron, Granisetron ,Dolasetron, Palonosetron • Substance P Antagonists (NK-1 Receptor Antagonists • Corticosteroids • Benzodiazepines: Lorazepam, Olanzapine • Phenothiazines: Prochlorperazine • Butyrophenones: Droperidol and haloperidol • Dopamine 2 Antagonists: Metoclopramide • Cannabis – don’t medically recommend to patients as a military physician
5-HT3 antagonists • Cornerstone of controlling acute nause/vomitting • Equally effective across older formulations • Few adverse effects – HA, constipation • Relatively convenient dosing • Lower efficacy for delayed type of nause/vomitting • Even the generic remain expensive • Palonosetron (Aloxi) • Longer half life -- 40 hours • Better against delayed n/v • Studies ongoing to determine whether or not it should be the 5-HT3 antagonist of choice
Neurokinin-1 (NK-1) antagonists • Aprepitant (Emend) • Oral drug only 125 mg po day 1, 80 mg po day 2-3 • Resulted in significant n/v improvement compared to dexamethasone alone or dexamethasone with 5-HT3 antagonist • Adverse events: Hiccups, dyspepsia • Very expensive --three tabs = $322 • CYP 450 3A4 inducer
Corticosteroids • Old drugs with unclear mechanism for controlling CINV • Best when used with other anti-emetics • Effective for acute and delayed CINV • Dexamethasone • 20 mg IV for highly emetogenic • 8-20 mg for less emetogenic • Continue PO daily or BID for 4 days • Methylprednisolone IV also used
Other adjunctive antiemetic • Benzodiazepine helpful in anticipatory n/v • Lorazepam used first line • Metoclopramide (Reglan) • Prochlorperazine (Compazine) • Dronabinol (Marinol) • Olanzapine (Zyprexa) • Has ODT formulation and may be helpful in sundowning inpatients with n/v
Breakthrough & Refractory Emesis • Challenging to reverse when preventive agents fails • Ensure adequate hydration and consider admission • Check and correct electrolyte imbalances • Use IV route and scheduled doses • May lead to anticipatory nausea/vomiting with next cycle if uncontrolled • For refractory emesis • Supportive care, hydration, nutritional supplementation • Strongly consider cessation/alteration of chemotherapy regimen
Think Outside the Box (TOB) • Could it be disease related • Brain mets • Bowel obstruction • Paraneoplastic effects (hypercalcemia, hyponatremia) • Radiation enteritis • Could it be new infection • Could other emetogenic meds like opioids be contributing?
Case – Hospital day 2 • Staff Sergeant Jones is feeling better with schedule anti-emetics, rehydration and correction electrolytes discovered on additional labs • She reports 5 episodes of diarrhea overnight with increasing dysphagia • Exam show normal vital signs and oral lesions with new sores on bilateral lips • Labs: LFT 2.5 x ULN, wbc 2.2, ANC 800, hgb 7.8, plt 30, Bun 35 sCR 1.5 • What the clinical issues now and how would you proceed?
Diarrhea • Major toxicity of several drugs used to treat gastrointestinal cancers such as 5-FU and irinotecan • Rule out infection before giving anti-motility agent – c-diff if at risk • Anti-Motility Drugs • Loperamide (Imodium) • Diphenoxylate (Lomotil) • Octreotide (Sandostatin) • Somatostatin analogue • Works to prolong GI transit time • Subcutaneous administration • Acute diarrheal reaction to irinotecan Atropine at time of treatment
Mucositis (Mouth Sores) • More common with certain drugs • 5-fluorouracil (5-FU) • Methotrexate • Doxorubicin (Adriamycin) • Cyclophosphamide (Cytoxan)
Mucositis • Prevention • Icing of the mouth during treatment • Treatment Options • Gel Clear • Magic Mouthwash • Viscous lidocaine • Narcotics • Maintain vigilance for both local viral and systemic infection
HEPATOTOXICITY • Etiology – many drugs and infection • CONSEQUENCES are many including suboptimal drug delivery, bleeding due to poor synthetic funciton and long term liver compromise • SURVEILLANCE - serum bilirubin, AlAt, AspAt, GGTP, NH3, PT/PTT - Liver u/s and biopsy as needed • PREVENTION - Dose adjustment to current liver function - Monitor infection with hepatotropic viruses (HBV, HCV)
RENAL TOXICITY • Classic nephrotoxic chemotherapy = platinum drugs (cisplatin, carboplatin, less so oxaliplatin) and methotrexate • PREVENTION - cisplatin – administration of magnesium sulphate, mannitol for diuresis induction and hyperhydratation - metotrexate – hyperhydratation, diuretics,urine alkalization - Avoid and discontinue concomittant nephrotoxin NSAIDS, IV contrast etc
Case – Hospital day 4 • Nurse reports to you that Staff Sergeant Jones has fever of 100.5 with chills • You give verbal stat orders for labs and xray • Nurse raises concern that you should come to ward and evaluate patient as the team just left • Your exam demonstrates an ill appearing pt shivering in bed. She reports to you that she is fatigued & her feet and hand “feels funny”. Temp is reported with BP 95/50 and HR 120. Severe mucositis is present. Lung and heart otherwise nl. Left upper arm picc line site is erythematous without exudate. • She has no other vascular access • STAT labs show LFT 3 x ULN, wbc 1.1, ANC 400, hgb 5.8, plt 18, Bun 35 sCR 1.3 • How would you proceed?
Case – Hospital day 4 • Clinical problems • Fatigue • Diarrhea • Neutropenic fever with unstable VS • Possible Catheter related line infection • Grade 3 Anemia and thrombocytopenia • Worsening mucositis – you’re dealing with this !! • Hepatic and renal dysfunction – you know this already !! • And what’s with the hyperpigmented feet and hand feeling funny?
Fatigue: Multifactorial • Anemia • Erythropoietin (Procrit)/darbepoetin (Aranesp) • Depression • Selective serotonin reuptake inhibitor (SSRI) • Sleep Disturbance -- Sleep aid: zolpidem tartrate (Ambien), eszopiclone (Lunesta) • Psychostimulants -- Methylphenidate (Ritalin)
Bone marrow suppression • Very common complication of chemotherapy • Has potential to cause mortality than any other complication • Leads to • Thromocytopenia – bleeding and more bleeding • Anemia – fatigue, cardiovascular and cerebrovascular events • Neutropenia – bacterial infection • Lymphopenia and hypogammaglobulinemia => risk of viral, fungal and protozoal infection
Neutropenic Fever • Neutropenic fever is a medical emergency • Infectious mortality in chemotherapy patients was 75% before empiric antibiotic therapy became the standard of care • Similar mortality (70% ) seen with a delay in administration of empiric antibiotics in patients with neutropenic fever • The Infectious Disease Society of America (IDSA) guideline provides best of expert advice -- last updated 2010
Duration and extent of bone marrow depression depends on drug
CHANGING PARADIGMS • Shift from Gram-positive to Gram-negative pathogens • New Gram-positive and Gram-negative • Increasing importance of fungi, especially Candida sp in neutropenic patients • Increasing incidence of resistant pathogens (MRSA, VRE, Candida) • Availability of G-CSF and GM-CSF • Development of broad spectrum antimicrobials • Early use of empiric antimicrobial therapy • Improved infection control • Use of prophylactic antimicrobial therapy remain controversial and not adviced
IDSA INITIAL ANTIBIOTIC CONSIDERATION • Only 23% of febrile neutropenic episodes are assocaited with bacteremia • Gram positive organism – 57% with 5% mortality • Gram negative organisms – 34% with 18% mortality • Polymicrobial –9% • The goal of initial empiric abx is to prevent serious mortality and morbidiy • Coverage of pseudomonas aeruginosa continues to drive initial antibiotic choices IDSA 2010 update accessed 1/3/12
IDSA INITIAL ANTIBIOTIC THERAPY CONSIDERATION • Negative blood cultures does not preclude empiric antibiotics in febrile neutropenic patients • May have occult infection • No clinical trial have shown superiority of one single empiric regimen • Ultimate selection should be based on • Whether patient’s risk is low vs high • Localizing infectious signs or symptoms – pulmonary infiltrates or cellulitis • Epidemiologic trends of pathogens causing infections in neutropenic patients • Special attention to local and individual patient patterns of bacterial colonization and resistance IDSA 2010 update accessed 1/3/12
IDSA INITIAL ANTIBIOTIC THERAPY CONSIDERATION • Drug allergies • Drug interactions • Organ dysfunction -- renal and liver IDSA 2010 update accessed 1/3/12
Initial management of fever and neutropenia—IDSA 2010 update
Initial management of fever and neutropenia—IDSA 2010 update
IDSA INITIAL ANTIBIOTIC THERAPY CONSIDERATION IDSA 2010 update accessed 1/3/12