Download
1 / 53
530 likes | 675 Vues
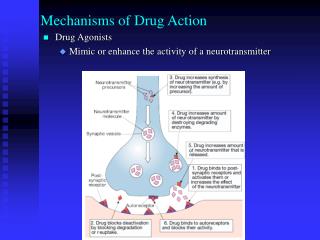
U.S. Department of Health and Human Services. National Institutes of Health. National Heart, Lung, and Blood Institute. BIOCHEMICAL MECHANISMS OF DRUG TOXICITIES. Lance R. Pohl, Pharm.D., Ph.D.

E N D
U.S. Department of Health and Human Services National Institutes of Health National Heart, Lung, and Blood Institute BIOCHEMICAL MECHANISMS OF DRUG TOXICITIES Lance R. Pohl, Pharm.D., Ph.D. Chief, Section of Molecular and Cellular Toxicology Laboratory of Molecular Immunology pohll@nih.gov 1/4/2007
Anaphylaxis Hemolytic anemia Granulocytopenia Thrombocytopenia Aplastic anemia Vasculitis Hepatic Skin Renal Pulmonary Cardiac Neurological Lupus TOXICITIES PRODUCED BY DRUGS
Heart disease Cancer Stroke Adverse drug reactions Pulmonary disease Accidents Pneumonia Diabetes Lazarou et al., JAMA, 279, 1208 (1998) 743,460 529,904 150,108 106,000 101,077 90,523 75,719 53,894 LEADING CAUSES OF DEATH IN USA IN 1994
TYPE A ADRs • Accounts for 80% of ADRs • Dose-dependent and often predictable • Often due to excessive expression of known pharmacologic effects • Often caused by drug-drug interactions • Often reproduced in animals Role of transporters in drug interactions, C.J. Endres, et al., European Journal of Pharmaceutical Sciences, 27, 501 (2006)
EXAMPLES OF TYPE A ADRS • Drowsiness from the use of antihistamines • Exacerbated therapeutic responses of warfarin and phenytoin-low therapeutic indices • Posicor, anti-hypertensive withdrawn from market because inhibited the metabolism of over 30 drugs • Acetaminophen • Fialuridine
FIALURIDINE-INDUCED MITOCHONDRIAL INJURY IN PATIENTS • FIAU is a uridine analog developed for hepatitis B treatment • Administration to 15 patients resulted in 7 developing severe mitochondrial liver damage with 5 dying and 2 receiving liver transplants • Toxicity was not predicted from rodent studies • Toxicity of FIAU is apparently due to FIAU-TP which inhibits mitochondrial DNA polymerase-γ and DNA synthesis • Humans and not rodents have human nucleoside transporter 1 (hENT1) in the mitochondrial membrane E.W. Lee, et al., J.Biol.Chem., 281, 16700 (2006)
TYPE B ADRs • Accounts for 20% of ADRs • Rare, unpredictable, and highly host-dependent • Mechanisms usually unknown, but in some cases they have been attributed to: • Allergic reactions • Pseudoallergic reactions • Deficiency in cytoprotective factors • Polymorphisms • Rarely reproduced in animals
ROLE OF IMMUNE SYSTEM IN INITIATING DRUG-INDUCED ALLERGIC REACTIONS
DRUG-INDUCED LIVER DISEASE IS A MAJOR HEALTH PROBLEM It is a major cause of acute liver failure and a major safety reason for: • Stopping preclinical development of drugs • Terminating clinical trials of drugs • Withdrawing drugs postmarketing F. Ballet, J. Hepatol., 26 (Suppl. 2), 26 (1997)
Antihypertensives Lipid-lowering agents NSAIDs Antimicrobials Antidiabetic agents Anticonvulsants Psychotropic agents Inhalation anesthetics Herbal medicines LIVER DISEASE IS CAUSED BY MANY COMMONLY USED CLASSES OF DRUGS
Iproniazid Ibufenac (Europe) Ticrynafen Benoxaprofen Perhexilene (France) Dilevalol (Portugal and Ireland) Bromfenac Troglitazone Nefazodone (Serzone) Ximelagatran (Exanta) 1956 1975 1980 1982 1985 1990 1998 2000 2003 2004 DRUGS WITHDRAWN / NOT APPROVED DUE TO LIVER DISEASE
COMPLEXITY OF DRUG-INDUCED LIVER DISEASE Initiation Progression Secondary Injury Repair Death Reactive Metabolites Innate Immune System Activation Kupffer Cells Protein Adducts Dendritic Cells ROS, RNS Injury NK and NKT Cells, Monocytes, PMNs, and Eosinophils Release of Protein Adducts Release of Adjuvants Adaptive Immune System Activation Effector Abs and T Cells
HALOTHANE HEPATITIS PATIENTS’ SERUM ANTIBODIES (% REACTIVITY)
OTHER FLUORINATED INHALATION ANESTHETICS FORM IDENTICAL PROTEIN ADDUCTS
Drug Tienilic acid Dihydralazine Ethanol Antigen CYP2C9 CYP1A2 CYP2E1, CYP3A4, CYP2E1-hydroxyethyl radical CYP AUTOANTIBODIES ASSOCIATED WITH OTHER DRUGS CAUSING ALLERGIC HEPATITIS
Cotrimoxazole Erythromycin Ketoconazole Ampicillin Allopurinol Ibuprofen Captopril -Methyldopa Enalapril Maria and Victorino, Gut, 41, 534 (1997) Chlorpromazine Amineptine Dothiepine Phenytoin Carbamazepine Tamoxifen Glibenclamide Lovastatin Propylthiouracil T CELL REACTIVITY ASSOCTIATED WITH DRUGS CAUSING ALLERGIC HEPATITIS
IL-10 DEFICIENCY INCREASES APAP-INDUCED LIVER INJURY AND DEATH
IL-10/iNOS KO MICE ARE NO MORE SUSCEPTIBLE TO APAP THAN WT MICE
IL-10 PROMOTER POLYMORPHISMS IN DRUG-INDUCED LIVER DISEASE • Diclofenac: G. P. Aithal et al., Gastroenterology, 118(4), 1077, Part 1, Supplement. 2. April 2000 • Ethanol: J. Grove et al., Gut 46, 540-545 (2000)
OTHER HEPATOPROTECTIVE FACTORS UNCOVERED WITH KNOCK OUT MICE • IL-6: liver regeneration, prevents apoptosis, induces HSPs • COX-2: prostaglandin products induce HSPs and prevent inflammation • IL-4 and IL-13: mechanisms not yet defined • Nrf2: regulates induction of GSH synthesis, UGTs, GSTs, NADPH quinone reductase, heme oxygenase, catalase • CCR2: down regulates INF-γand TNF-α Y. Masubuchi K. Chan, et. al., PNAS, 98, 4611 (2001);C.M. Hogaboam, et. al., Am. J. Pathol., 156, 1245 (2000).
NIH FUNDS NETWORK TO STUDY DRUG-INDUCED LIVER INJURY (DILIN) • Sponsored by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) in 2004 • The DILIN centers are located at U. of North Carolina, Duke, U. of Michigan, U. of Connecticut, and U. of California in SF • The goal is to establish a registry of patients who have experienced severe drug-induced liver disease and collect biological samples for biochemical, serological, and genetic testing by investigators throughout the country
DRUG-INDUCED CUTANEOUS ADRS • Exanthems-95% are erythematous or maculo-papular in nature and are usually self-limiting when the drug is withdrawn, Steven-Johnson syndrome and toxic epidermal necrolysis are life-threatening • Exanthems from β-lactam antibiotics are often mediated by drug-specific IgE antibodies while many others by CD4+ and CD8+ T cells N. Yawalkar, Toxicology, 209, 131(2005)
T CELL REACTIVITY TO DRUGS CAUSING CUTANEOUS ADRS • Lidocaine • Sulfonamides • -Lactam antibiotics • Phenytoin • Carbamazepine Lebrec et al., Cell Biology and Toxicology, 15, 57 (1999)
MECHANISM OF T-CELL MEDIATED CUTANEOUS ADRS S. Roychowdhury and. C.K. Svensson, The AAPS Journal, 7, E834 (2005)
Alcuronium Cephalosporins Penicillins Protamine Streptokinase Park et al., Chem. Res. Toxicol., 11, 969 (1998); B.Y.H. Thong and Y. Chan, Ann. Allergy Asthma Immunol., 92, 619 (2004). Sulfamethoxazole Suxamethonium Thiopentone Trimethoprine Tubocurarine IgE-MEDIATED ANAPHYLACTIC DRUG REACTIONS
ASSOCIATION OF GENETIC VARIANTS OF HLA-B AND HSP70 WITH HYPERSENTIVITY TO ABACAVIR • Abacavir is a nucleoside reverse transcriptase inhibitor used to treat HIV type 1 • Approximately 5% of patients who receive abacavir develop a treatment-limiting hypersensitivity reaction, characterized by fever, rash, gastrointestinal symptoms (nausea, vomiting, diarrhea or pain) and lethargy or malaise • Median time to onset is 11 days, but symptoms occur within hours when patients are rechallenged • Susceptibility is associated with specific variants of HLA-B and HSP70 and CD8+ T cells that are activated in presence of abacavir to produce TNF A.M. Martin, et. al., PNAS, 101, 4180 (2004)
PSEUDOALLERGIC (ANAPHYLACTOID) REACTIONS WITH NSAIDS • Most cases occur with aspirin, although other NSAIDs can be involved except for COX-2 inhibitors • Reactions include asthma, rhinitis, urticaria and/or anaphylactic shock. • Not mediated by IgE antibodies • COX-1 inhibitors may divert arachidonic acid metabolism to 5-lipoxygenase pathways and formation of proinflam-matory cysteine-leukotrienes
PSEUDOALLERGIC (ANAPHYLACTOID) REACTIONS WITH NSAIDS • Leukotrienes cause bronchial smooth muscle contraction, mucous secretion, vasodilation, and cellular infiltration • Cysteine-leukotriene receptor 2 poly-morphisms associated with aspirin intolerance J.S. Park et al., Pharmacolgenics and Genomics, 15, 483 (2005)
ANAPHYLACTOID REACTIONS WITH IODINATED RADIOCONTRAST AGENTS • Reactions can be similar to aspirin and include asthma, rhinitis, urticaria, gastrointestinal symptoms, and/or anaphylactic shock consisting of hypotension, pulmonary edema, respiratory arrest, cardiac arrest, and convulsions • Mechanisms? J. Szebeni, Toxicology 216, 106 (2005)
ENZYME POLYMORPHISMS AND TYPE B ADVERSE DRUG REACTIONS • Sensitivity to warfarin and phenytoin due to metabolic deficiency caused by CYP2C9*3 Rettie et al., Epilepsy Research, 35, 253 (1999); Brandolese et al., Clin. Pharmacol. Ther., 70, 391 (2001) • Irinotecan side effects of serious and potentially fatal diarrhea and neutropenia are associated with metabolic deficiency caused by UGT1A1*28 and other allelic forms of UGT1A Han et al., J. Clin. Oncol., 24, 2237 -2244 (2006)
THIOPURINE-S-METHYLTRANSFERASE POLYMORPHISMS AND TYPE B ADR • Thiopurine drugs 6-mercaptopurine and aza-thioprine are used to treat acute lymphoblastic leukemia in children, inflammatory bowel disease, autoimmune disease, and organ transplant recipients • Polymorphisms of TPMT that lead to low enzyme activity result in life-threatening pancytopenia L. Wang and R. Weinshilboum, Ongene, 25, 1629-1638 (2006)
THIOPURINE METABOLISM RESULTS IN THERAPEUTIC ACTIVITY AND TOXICITY
DRUG-INDUCED-LONG QT SYNDROME • Results in prolonged ventricle repolarization that can lead to polymorphic ventricular tachycardia (torsade de pontes), and ultimately ventricular fibrillation and death • Rare, unpredictable, and a major reason for withdrawal or restriction of many drugs • Antiarrhythmic drugs such as quinidine, procainamide, sotalol and others • Other classes of drugs cause this syndrome including astemizole (antihistamine), terfenadine (antihistamine), mibefradil (anti-hypertensive), and grepafloxacin (antibiotic) • Linked to genetic variants of drug-metabolizing enzymes • Linked to cardiac K ion channel subclinical mutations P.J. Kannankeril and D.M Roden, Current Opinion in Cardiology, 22, 39 (2007)
Summary • Drug-drug interactions are a major cause of Type A ADRs and are in many cases predictable • Type B ADRs may be caused by rare allelic forms of enzymes, receptors, ion channels, transporters, transcription factors, etc • Many Type B ADRs also appear to be mediated by specific Abs and T cells that are induced by protein adducts of reactive metabolites • It is likely that numerous factors protect most people from getting Type B ADRs and rare polymorphisms of one or more of these factors determine individual susceptibility • Toxicogenomics and proteomics should provide new information about other important regulatory factors that normally protect cells from TYPE B ADRs
REFERENCES Incidence of adverse drug reactions in hospitalized patients - A meta-analysis of prospective studies, J. Lazarou, et al., J. Am. Med. Assoc. 279, 1200 (1998). The epidemiology of serious adverse drug reactions among the elderly, P. A. Atkin, et al., Drug Aging, 14, 141 (1999). Postmarketing surveillance and adverse drug reactions - Current perspectives and future needs, T. Brewer and G. A. Colditz, J. Am. Med. Assoc. 281, 824 (1999). Computerized surveillance of adverse drug reactions in hospital: Implementation,M. Levy, et al., Eur. J. Clin. Pharmacol., 54, 887 (1999). Retrospective analysis of the frequency and recognition of adverse drug reactions by means of automatically recorded laboratory signals, I.Tegeder, et al., Brit, J. Clin. Pharmacol. 47, 557 (1999).
REFERENCES Mechanisms, chemical structures and drug metabolism, L. R. Pohl, et al., Eur. J. Haematol., 57, 98 (1996). Allergic and autoimmune reactions to xenobiotics: how do they arise?, P. Griem, et al., Immunol.Today, 19, 133 (1998). Role of drug disposition in drug hypersensitivity: A chemical, molecular, and clinical perspective, B. K. Park, et al., Chem. Res. Toxicol., 11, 969 (1998). Covalent binding of xenobiotics to specific proteins in the liver, N. R. Pumford et al., Drug Metab. Rev., 29, 39 (1997). Halothane-induced liver injury in outbred guinea pigs: Role of trifluoroacetylated protein adducts in animal susceptibility, M. Bourdi et al., Chem. Res. Toxicol., 14, 362 (2001). The role of leukocyte-generated reactive metabolites in the pathogenesis of idiosyncratic drug reactions, J. P. Uetrecht, Drug. Metab. Rev., 24, 299 (1992).
REFERENCES Characterization of the humoral immune response and hepatotoxicity after multiple halothane exposures in guinea pigs, M. Chen and A. J. Gandolfi, Drug Metab. Rev., 29, 103 (1997). Human cytochrome P450 2E1 is a major autoantigen associated with halothane hepatitis. M. Bourdi, et al., Chem. Res. Toxicol. 9,1159 (1996). Cytochromes P450 and uridine triphosphate glucuronosyl-transferases: Model autoantigens to study drug-induced, virus-induced, and autoimmune liver disease, M. P. Manns and P. ObermayerStraub, Hepatology 26. 1054 (1997). Structure-activity studies in drug induced anaphylactic reactions, B. A. Baldo and N. H. Pham, Chem. Res. Toxicol., 7, 703 (1994). Mechanisms of drug-induced allergic contact dermatitis, H. Lebrec, et al., Cell Biol. Toxicol. 15, 57 (1999).