Project P.I.E.
Project P.I.E. . Brita Brown, MSW, Community Organizer Nona Moscovitz, MSW, Program Manager Mental Health Services Kareen Nour, Ph.D. Researcher Marijo Hébert, Research assistant. Project P.I.E. Presentation of the project Evaluation of the project. Disclosure.

Project P.I.E.
E N D
Presentation Transcript
Project P.I.E. Brita Brown, MSW, Community Organizer Nona Moscovitz, MSW, Program Manager Mental Health Services Kareen Nour, Ph.D. Researcher Marijo Hébert, Research assistant
Project P.I.E. • Presentation of the project • Evaluation of the project
Disclosure • The author of this presentation has no conflicts that have a direct bearing on the subject matter of this presentation.
Project P.I.E. • Presentation of the project
Mental health and older adults • 1/5 of older adults lives with a mental health problem. • This number will double by 2030. • 50% of older adults living with a mental health problem do not receive services related to this problem. • They are among the most vulnerable of society and represent a high risk group. • Long-term impact on the health care system. • Their quality of life is compromised.
Three aspects of the project • Prevention • Tap into the community and use its available resources to reach out to those most vulnerable. • Intervention • Offer assistance even before it is sought. • Education • Counter long-standing prejudices against society’s most vulnerable members.
Objective • Identify vulnerable and/or isolated older adults in the community who are living with a mental health problem with or without another existing condition such as a chronic or debilitating illness and who hesitate or cannot ask for the services they might require. • Refer to the appropriate services.
Goals • For the clientele: • Maintain autonomy • Improve quality of life • Prevent a potential crisis • Prevent a premature hospitalization and/or long term placement • For the community: • Build, on a wider scale, a sense of belonging to one’s community
Gatekeeper Model • Origin: • Spokane, Washington 1978. • Characteristics: • Non traditional referral sources: the Gatekeepers • Proactive outreach. • Efficiency of the model: • 41% of referrals made to services provided to seniors came from Gatekeepers. • Older adults referred by the Gatekeepers were different from those referred by traditional sources of referral.
Adaptation of the model • Health and social services system of Québec. • Urban environment. • Referral model based on self-referral and empowerment. • Involvement of volunteers to train the Community Liaisons. • Volunteers receive a training by the CSSS so they can be trainers.
Community Liaisons Who are they? • Individuals who come into contact with vulnerable or isolated older adults by way of their occupation and/or daily activities. • Have frequent, ongoing contacts with the target population or have established a friendly or cordial relationship with it. • Non traditional sources of referral (bank tellers, superintendents, grocery clerks, hairdressers, etc.). • Agree to have a brief training on the detection of risk behaviors exhibited by the target population.
Older adults reluctant or resistant to seek assistance They may…. • be embarrassed by their situation. • be afraid of losing their dwelling through eviction or placement. • want to avoid being a burden on family, friends or neighbours. • downplay or deny that they are ill and in need of any assistance. • be fearful of losing their independence. • be experiencing a significant loss or depression.
Risk-behaviors (PARBAS Assessment tool) • Self-Neglect • Poor personal hygiene – body odours, poor nutrition, inappropriate clothing for the weather, etc. • Non-compliance • Refusal to accept assistance for reduced functioning, etc. • Substance abuse: • Many outdated prescription pill bottles, many empty alcohol bottles, etc • Compromised security • Irritable, angry or hostile, increased withdrawal. • Indiscriminately discloses their financial situation to others, etc. • Financial security • Excessive spending, difficulty in meeting financial obligations, unpaid bills.
Risk behaviours • Changes in behaviour • Aggressive, verbal and/or physical behavior directed toward self / others / property, appears agitated and fidgety. • Emotional distress • Complaints of no appetite or of not sleeping, avoids any communication, and has little or no social contacts. • Suicidal behaviour • Thoughts or plan of suicide, giving away personal possessions or putting personal affairs in order, etc. • Victim of mistreatments • Withdrawn and timid, insulted by others, cuts on body, large sums of money withdrawn from bank account, etc.
Community Liaisons Their role • To be able to recognize the different signs and behaviours that indicate that a vulnerable or older adult is in need of some assistance. • To be a link between the client and the CSSS. • They inform them of the existence of available services. • They encourage them to self-refer and, if necessary, assist them in the referral process.
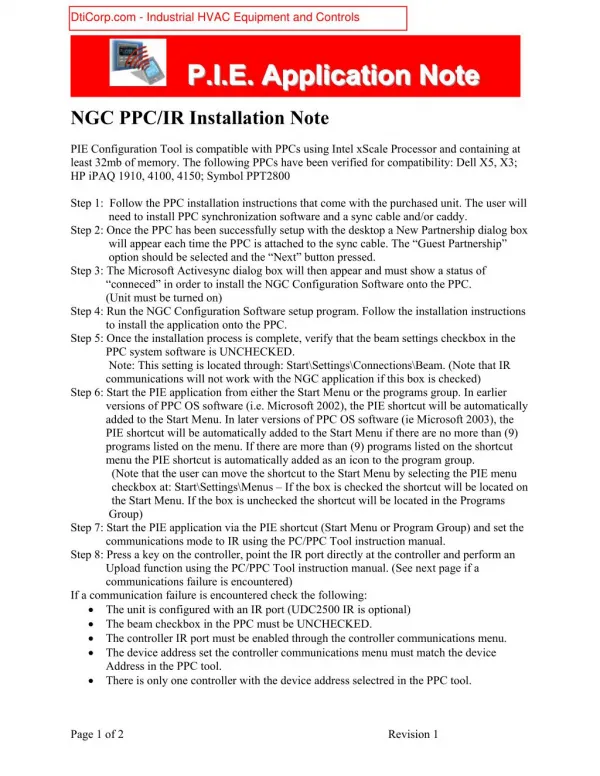
Referral process 1. Self referral • The Community Liaison gives a ProjectP.I.E. business card to the individual. • The individual calls the ProjectP.I.E. line or shows up at the psychosocial intake. • In the case where the individual shows up at the CSSS, the intake worker verifies if it’s a referral through Project P.I.E. • The intake worker gathers nominative information and evaluates the situation. • If necessary, the file is transferred to the relevant CSSS program.
2. Referral by a Community Liaison The Community Liaison calls the ProjectPI.E. line or shows up at the psychosocial intake and mentions that it is a referral through ProjectP.I.E. Provides the person’s name, address, and telephone number. Describes his or her concerns and relates the risk behaviours. Specifies if the person has, or not, any support system such as family, friends, neighbours. Gives his or her name and telephone number, although if the Liaison wishes to remain anonymous, it will be respected. The intake worker evaluates the situation and transfers, if required, the case to the relevant CSSS program.
Consent The consent of the older adult is required to communicate information regarding his or her situation but may be waived in specific situations. • Potential danger to oneself or others; • Not able to fully consent (incapacitated).
Confidentiality Both the Community Liaison and the vulnerable or isolated older adult have the right to have information provided kept confidential.
Ethical considerations • Vulnerable or older adults have a right to be informed of alternatives and options. • Community Liaisons : • do not interfere nor violate an older adult’s right to privacy; • do not try to impose services upon them; they respect the decision of the older adult to contact, or not, available services; • can serve as a link between the older adult and the CSSS.
Project P.I.E. • Evaluation of the project
Evaluation framework • Few evaluation frameworks exist in mental health for screening or for outreach programs. • Eight criteria were analysed and three of them were retained: they correspond to the three objectives of the evaluation.
Criteria for a reliable health screening program 1.Disease: relevance of the problem. • 1/5 of older adults lives with a mental health issue. • Vulnerable and can represent a danger for themselves or others. • Treatment: for each screened client, there should be an existing and accessible treatment and follow up. • Outreach program : the efficacy of the program to screen isolated or vulnerable older adults living with a mental health problem (to be evaluated).
Criteria for a health screening program • Screener: the capacity of Community Liaisons to screen: the relevance of the training offered to the Liaisons and to the trainers (to be evaluated) • Target population : screening for a population in need not receiving services. • half of older adults living with a mental health problem. • Facing social, emotional, physical, financial or organizational barriers. • Exhibiting self-neglect or socially isolated.
Criteria for a health screening program • Efficacy of treatment: the mental health team of the CSSS Cavendish can offer a psychosocial intervention. • The intervention is offered by a multidisciplinary team and is based on an at-risk behaviour approach. • Cost-efficacy score: number of screened vulnerable and/or isolated older adults versus costs related to implementing outreach program (to be evaluated).
Criteria for a health screening program • Sustainability of the program: In order to improve and sustain this outreach program (Project P.I.E.), periodic revisions will be made according to the results obtained by the research evaluation.
Study • This is an longitudinal exploratory study (nine month pilot study), where information is gathered and evaluated at different intervals: from March 2007 to December 2007.
Objective #1 • Is to evaluate the efficiency of Project P.I.E in order to identify older adults that are vulnerable or isolated and that live with a mental health problem. How: • Number of referred people at risk • Information on the various referral processes • Demographic information and health profile • Cost-efficacy
Referred people at risk (three month period): 1. Self-referral: Through the P.I.E. line = 1 In person at the CSSS = 1 2. Referral by a Community Liaison: Through the P.I.E. line = 3
Information on the various referral processes • Qualitative information collected by intake workers show the following obstacles: • Some referrals are undereported as P.I.E. calls or walk-ins (referral source is not mentioned during the initial screening process). • Individuals referred by Liaisons are not necessarily living in the territory served by the CSSS Cavendish.
C. Demographic information and health profile • Age = represented in each age category: from under the age of 46 to 89. • Gender • Male = 40% • Female = 60% • Civil Status (4 out of 5 respondents) • Married or common law = 25 % • Widow(er) = 25 % • Single = 50% • Type of dwelling (4 out of 5 respondents) • Alone = 50% • In couple = 25% • With someone else = 25%
C. Demographic information and health profile cont’d… • Major clinical profile: • Physical = 20% • Psychological = 60% • Physical and Psychological = 20% • CSSS Program providing services: (4 out of 5 respondents) • Mental health program = 50% • PALV= 50%
Objective #2 • Is to document the implementation of Project P.I.E. How: • Training sessions. • Community’s response to the Project.
A. Training sessions 1) Trained individuals: Trainers = 6 Community Liaisons trained = 117 Community liaisons trained who answered the questionnaires = 108
B. Community’s response to the Project • Organizations who accepted a training= 32 • Trainings offered= 18 • Older adults that frequent the organization on a regular basis = 70% • Organizations who refused the training = 24
3.Geographic areas of the organizations on the CSSS territory NDG = 10 Snowdon Ouest = 1 Côte St-Luc = 7 4. Trainers who received the training Total = 6 Volunteers = 2 Students = 2 Workers = 2
Objective #3 • To document the feeling of community solidarity felt by the principal actors of ProjectP.I.E. (trainers and Community Liaisons).
Feeling of solidarity for the Community Liaison: Following the training (scale from 1 to 5) Level of confidence to give information card to the target population = 4.02 (1.02) Feeling of involvement towards the community= 3.84 (1.02) Level of awareness related to Mental health issues/challenges= 3.91 (1.03) Existing prejudices, etc. = 3.55 (1.13) Feeling of usefulness in helping a vulnerable and/or isolated population = 3.96 (.97)
Feeling of solidarity for the trainers: Following the training (scale from 1 to 5) Level of confidence to train Community Liaisons = 4.50 (.57) Feeling of involvement towards the community= 4.00 (.81) Level of awareness related to Mental health issues/challenges= 4.75 (.50) Existing prejudices, etc. =5.00 (.00)