Download
1 / 49
490 likes | 535 Vues
PLH - 419. Topics 1. General Principles of Toxicology, 2. Management of the Poisoned Patient, 3. Teratogenesis. By Dr. Sabry Attia Professor of Pharmacology and Toxicology. General Principles of Toxicology. Defination of toxicology. Purposes of toxicology.

E N D
PLH - 419 Topics 1. General Principles of Toxicology, 2. Management of the Poisoned Patient, 3. Teratogenesis By Dr. Sabry Attia Professor of Pharmacology and Toxicology
General Principles of Toxicology • Defination of toxicology. • Purposes of toxicology. • Terms of toxicology ( Toxin, Toxicant and Poisons). • Classification of toxic agents (Target organs, use, source, effects, physical state, chemical stability, chemical structure, poisoning potential, biochemical mechanisms of action). • Development of toxicology (especially after the widespread use of anaesthetics, disinfectants, radioactivity, vitamins). • The tragic of thalidomide incident. A toxicologist is trained to examine the nature of toxic agents effects including their cellular, biochemical and molecular mechanisms of action and assess the probability of their occurrence.
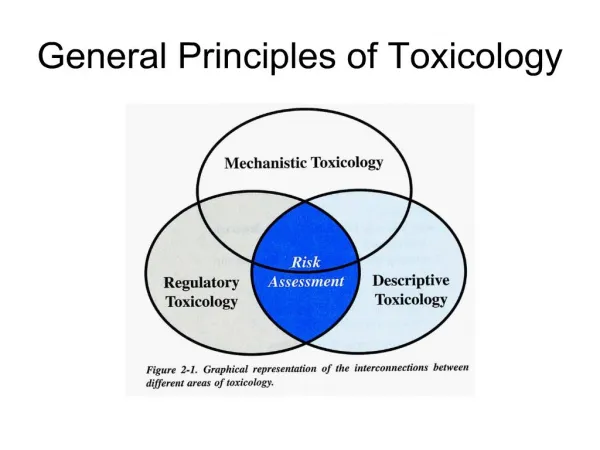
Branches of Toxicology Categories • Descriptive toxicologist. • Mechanistic toxicologist. • Regulatory toxicologist. Other specialized areas; • Occupational (Industrial) toxicology. • Environmental toxicology. • Ecotoxicology. • Forensic toxicology. • Analytical toxicology. • Clinical toxicology.
Exposure and Toxic Responses • Exposure classes (toxicants in food, air, water, and soil as well as toxicants characteristic of domestic and occupational settings). • Toxic effects may be systemic or local at the site of exposure. • The target organs that are affected may vary depending on dosage and route of exposure. • Sings and symptoms are the effects produced by the action of a particular poison on the physiological function of the body. • Certain general symptoms suggested the possibility of a number of poisons; • Sudden death (aconitine, cyanide and barium compounds). • Eyes (ergot, morphine, pilocarpine, atropine and cocaine). • Breath (acetic acid, ammonia, phenol, ether and iodine). • Mouth (atropine, pilocarpine and ammonia).
Exposure and Toxic Responses (cont.) • Skin (atropine, pilocarpine, strong acids and alkalies, cyanosis produced by aniline, acetanilide). • GIT (metals, ergot and food poisons). • Cardiovascular system (quinidine, digitalis, ephedrine and reserpine). • Liver (carbone tetrachloride and chloroform). • Kidney (phenol and sulphonamides). • Nerves (peripheral neuritis due to antimony and arsenic). • Skeletal muscle (curare and flaxedil). • Blood changes (anaemia by benzene, haemolysis due to saponins, leukopenia by benzene). • CNS (strychnine, picrotoxin, barbiturates, ether, alcohol).
Mechanism of Cellular Injury • Exposer to injurious agents or stress → reversible/irreversible cell injury → cell death. • Death of cells occurs in two ways: • Necrosis (irreversible), changes produced by E digestion of dead cellular elements. • Apoptosis (vital process that helps eliminate unwanted cells), an internally programmed series of events effected by dedicated gene products. • Toxicity can result from adverse changes such as: • Alteration of a cell membrane permeability: through interaction with its component as; • SH-containing proteins + HMs→ change in protein structure. • Lipids + Free radicals → lipid peroxidation. E.g. CCl4 metabolites (i.e. CCl3; CCl3OO.) radical causes lipid peroxidation and finally lead to liver necrosis. • Na-K ATPase pump inhibition → ↓ major AA and Ca2+ transport. E.g. HMs and alcohol. • Chang in enzyme activity: • Inhibition e.g. AchE inhibitors → ↑ A.Ch. CN- inhibits cytochrome oxidase enzyme → no aerobic respiration → cell death. • Activation e.g. Barbiturates induce HME →↑conversion of some non carcinogenic agents as Benzo(α)pyrene(in cigarette smoke) into carcinogenic ones.
Mechanism of Cellular Injury (cont.) • Interferance with co-enzymes: E.g.: CN- binds to essential metals as Fe3+ needed for the activity of cyochrome oxidase. • Modification of carriers: CO binds with Hb instead of O2 → carboxyhemoglobin→hypoxia • Formation of reactive metabolites: Benzo(α)pyrene (in cigarette smoke) is metabolized by HME to form a number of metabolites that may elicit its carcinogenicity. • Reactions causing depletion of GSH: As in paracetamol toxicity. • Action on nucleic acids: The metabolites of the air pollutions as SO2, NO2, NO, CO and O3 causing damage to DNA & mutation. • Disruption of protein synthesis: Some toxicants either increase or decrease protein synthesis leading to cellular injury. E.g.: Ricin (castor beans) getting inside the cells of a person's body and preventing the cells from making the proteins they need. • Lysosomal changes:labialization of the suicide bags by toxicants as HMs increase lysosomal membrane permeability → release of hydrolases → cell death. Moreover, stabilization of lysosomal enzymes bags by toxicants as Corticosteroids causes’ indirect toxicity by decreasing the response of the body defence mechanism.
Factors That Influence Toxicity • Physicochemical composition of the toxicant (solids, liquids, particle size, pH), • Dose and concentration (aspirin tablets, dilution), • Routes of administration (inhalation > IV > IP > SC > IM > ID > oral > topical), • Metabolism of the toxic agent (more polar or more toxic), • State of health (person with severe hepatic or renal disease, hypertension, head injuries), • Age and maturity (gray-baby syndrome, reduced pharmacokinetics in elderly people), • Nutritional state and dietary factors (stomach contents, types of food, proteins), • Pharmacogenetics or idiosyncrasy(succinyl-choline, aspirin, fava beans), • Sex (erythromycin, lipid sol., larger BV and tissue mass in men which dilute the chemical), • Environmental (temperature, occupation (liver-metab), living conditions), • Chemical interactions(the increase or decrease of toxicity by simultaneous or consecutive exposure to another one).
Evaluation of Safety of Chemicals and drugs Sources of information on safety • Experimental studies • Controlled clinical studies • Epidemiological studies Experimental studies • Goals of toxicity studies. • Adv. & disadv. of toxicity tests using experimental animals. • Characteristics of ideal animal species. • Examples. • Strains of rats 1. Specific pathogen free animals, 2. Germ free animals, 3. Dirty animals, 4. Rats for specific purposes.
Acute toxicity tests: Toxicometric studies LD50: Median lethal dose (the dose that causes 50% mortality in a population). LC50: Median lethal concentration (inhaled drugs). LD0: Represents the dose at which no individuals are expected to die. This is just below the threshold for lethality. LD10: Refers to the dose at which 10% of the individuals will die. EDs: Effective Doses that are used to indicate the effectiveness or harmful effect (paralysis) of substances. TI: The Therapeutic Index(is used to compare the therapeutically effective dose to the toxic dose = LD50 / ED50).
Acute toxicity tests: Toxicometric studies (cont.) Factors affecting LD50. • Species, age, sex, body weight, general health condition, strain, diet, nutritional status & number of animals used in the test • Route of administration (oral route differ from parental route) • Environmental conditions (lab conditions) i.e. intra & inter laboratory conditions • Experimental procedure, stress, dosage formulation. Importance of LD50: Classification of chemicals according to LD50 of drugs given orally to rats into; • Super toxic chemicals: LD50 < 5 mg/kg • Extremely toxic chemicals: LD50 = 5 – 50 mg/kg • Very toxic chemicals: LD50 = 50 – 500 mg/kg • Moderately toxic chemicals: LD50 = 0.5 – 5 g/kg • Slightly toxic chemical: LD50 = 5 – 15 g/kg • Practically non- toxic compound: LD50 > 15g/kg
Acute toxicity tests: Toxicometric studies (cont.) • The use of ED50 and LD50 doses to derive the TImay be misleading as to safety, depending on the slope of the dose-response curves for therapeutic & lethal effects. • Knowledge of the slope is important in comparing the toxicity of various substances. • For some toxicants a small increase in dose causes a large increase in response (toxicant A, steep slope). For other toxicants a much larger increase in dose is required to cause the same increase in response (toxicant B, shallow slope). • To overcome this deficiency, toxicologists often use another term to denote the safety of a drug - the Margin of Safety (MOS). • The MOS is usually calculated as the ratio of the dose that is just within the lethal range (LD01) to the dose that is 99% effective (ED99). The MOS = LD01/ED99.
Acute toxicity tests: Toxicometric studies (cont.) • NOAEL is the highest data point at which there was not an observed toxic or adverse effect. • LOAEL is the lowest data point at which there was an observed toxic or adverse effect. • The terms NOELs and LOELs do not necessarily imply toxic or harmful effects and may be used to describe beneficial effects of chemicals as well.
Acute toxicity tests: Skin & eye studies (Dermal) • Such testing may provide information on the adverse effects resulting from a dermal application of a single dose of a test substance. • The acute dermal test also provides the initial toxicity data for regulatory purposes, labelling, classification & subsequent subchronic & chronic dermal toxicity studies. • Comparison of acute toxicity by the oral & dermal route may provide evidence of the relative penetration of a test material. • Draize test • It is a simple and generalized test developed to study eye irritation in rabbits. • It is used as the animal test to identify human eye irritants. • The Draize test can adequately identify most of the moderate to severe human eye irritants
Acute toxicity tests: Pyramidal single dose test • Large number of dogs ≈ 100 are given a single daily X dose of a compound under test. • At the end of the day, the number of dogs which died & those which survived is observed. • The procedure is continued, till all dogs die, then plotting is done. • It helps in studying the mechanism of drug toxicity. • It can be used to determine any pathological changes by examination of the animal after death. • The effect of the drug on all body organs can be examined. • Clinical chemical tests can be performed on living animals (hematology, and detection of different biotransformation and excretion product (metabolites), and determination of t½ of the compound).
Prolonged toxicity studies • They predict any cumulative effect of the drug. • Compound under test is given daily in 3 dose levels for 2 – 4 weeks (Subacute), for 90 days (Subchronic) or more than 90 days (Chronic). • Animals are observed for different parameters: physiological, clinical and chemical tests, behaviour, CNS & autonomic profiles. • At the end of the test, animals are subjected to the following tests & then are killed. • Hematological studies: hemoglobin, RBCs, WBCs, platelets. • Clinical chemistry studies: serum creatinine, ALT, AST. • Histopathological studies:for different organs (spinal cord, heart, kidney). • Life – Span Toxicity Test • The same previous procedures are applied but treatment with chemicals starts after weaning of offsprings (litters). • Administration of the chemical is continued till death of animals. • When animals die spontaneously, the same previous parameters are determined.
Specific Toxicity Studies: • Reproductive toxicity (toxicity on male or female reproductive system) Toxic effects may cause: Decreased libido and impotence, Infertility, Interrupted pregnancy (abortion, fetal death, or premature delivery), Infant death or childhood morbidity, Altered sex ratio (fewer boys are born to fathers with high dioxin levels than expected) and multiple Births (Clomiphene), Chromosome abnormalities and Childhood cancer. • Developmental Toxicity (toxicity on developing embryo or fetus) Embryolethality (Failure to conceive, spontaneous abortion), Embryotoxicity (Growth retardation or delayed growth of specific organ systems), Teratogenicity (Irreversible conditions that leave permanent birth defects in live offspring). • Carcinogenic studies Carcinogenicity is a complex multistage process of abnormal cell growth and differentiation which can lead to cancer. The initial neoplastic transformation results from the mutation of the cellular genes that control normal cell functions. Mutation may lead to abnormal cell growth. It may involve loss of suppresser genes that usually restrict abnormal cell growth. Many other factors are involved (e.g., growth factors, immune suppression, and hormones).
Principles in management of Poisoned Patient Necessary measures to prevent further deterioration of the patient; • Stabilization of the patient, • Diagnosis of the poison, • Prevention and treatment of poisoning, • Administration of antidotes (specific antidotes or using the antidote cocktail), • Continuing care. 1. Stabilization of the patient (ABCDEs measures) • Evaluation of Airway obstruction Causes (Mucosal swelling, Secretions, Posterior displacement of the tongue and Foreign bodies). Signs and Symptoms (Dyspnea, Dysphoria, Air hunger, Cyanosis, Diaphoresis and Tachypnea). Measures (Clearing the airway, use of nose-pharyngeal tube, Intubation or Crico-thyroidotomy). B. Evaluation of Breathing Causes (Respiratory depressant drugs, Pneumonia, Pulmonary edema, Lung abscess, Pulmonary emboli, Bronchospasm from numerous environmental & occupational sources and Tetanus). Signs and Symptoms (Tachypnea, Cyanosis, Respiratory depression and altered mental state). Evaluated by measuring of blood gases (PaCO2, PaO2), Chest X-ray, or Tidal volume. Measures (Assisted ventilation and supplemental O2 delivered by nasal catheters and cannulae).
Principles in management of Poisoned Patient(cont.) C. Evaluation of (C) Circulation Signs and Symptoms of inadequate tissue perfusion is shock (Depressed consciousness, Decreased blood pressure, Peripheral vasoconstriction, Metabolic acidosis and Oliguria). Ranged from anxiety and tachycardia → delirium and coma. Treatment (Position change, Vasopressors as Dopamine and NE, and Fluids). D. Evaluation of Depression (D) or Excitation(E) • Depression is evaluated by (measuring the pupillary size, pupillary light reflex, motor responses to pain, and /or spontaneous eye movements). Treatment of depressed patient (coma cocktail: Glucose, Thiamine & Naloxone). • Excitation is manifested as seizures. Treatment of generalized seizures secondary to toxins (Diazepam, Phenytoin, Phenobarbital, General anaesthesia, pyridoxine, Hemodialysis, correction of the causes of altered body homeostasis as hypocalcemia, hypoxia, hypoglycaemia, meningitis, ---). • Treatment of violent patient duo to Toxins and conditions include (Benzodiazepines with Haloperidol and stabilization of blood glucose level).
Principles in management of Poisoned Patient(cont.) 2. The diagnosis of poisons Once the patient has been stabilized, the potential poison has to be identified. The diagnosis of poisoning involves the following; • History given by the patient himself or relatives. • Physical examination of the patient. • Laboratory investigations. I. History Adults (Conscious or unconscious patients). Children (presence of traces, disintegrated tablets, abnormal behaviour or GIT disturbances). II. Physical examination of the patient (Blood pressure, pulse, respiration, temperature, eyes, mouth, skin, abdomen, nervous system). III. Laboratory investigations. • Most laboratories limit drug screens to those substances commonly involved in poisonings. • Toxicant extraction from Urine, Blood, Hair, Meconium, Saliva or Sweat samples can be screened by TLC, GLC, GC-MS, Enzyme-mediated immunoassay techniques.
Principles in management of Poisoned Patient(cont.) 3. Prevention and treatment of poisoning A- Non ingested poison 1. Inhalation exposures • Immediate, cautious removal of the patient from the hazardous environment. • Administration of 100% humidified O2, assisted ventilation, and bronchodilators. • Observe for edema of the respiratory tract and later non-cardiogenic pulmonary edema. • Arterial blood gas assays, chest examination, and blood tests for the criminal substance (e.g., cyanide) should be performed. • Treatment should not await laboratory results. 2. Dermal exposures • Attendees should wear protective gear (gloves, gown, shoe covers). • Remove the patient’s contaminated clothes, contact lenses, and jewelry immediately. • Gently rinse and wash the skin with copious amounts of water for at least 30 minutes. • Do not use forceful flushing in a shower. Use slightly cold water and soap of oily substances. • Toxic substances such as organophosphorous compounds, metal compounds, phenol, may penetrate the intact skin and must be handled with proper protective equipment. 3. Ocular exposures • Ocular decontamination consists of at least 15 minutes of immediate irrigation of eyes with normal saline or water. Alkaline or acid irrigating solutions should be avoided. • Continue to irrigate the eye for as long as the pH is abnormal. • Alkaline corneal burns are requiring ophthalmic consultation.
Principles in management of Poisoned Patient(cont.) B- Ingested poison 1- Dilution of the poison with water and milk (demulcent). 2- Prevention of further absorption of poison. • Induction of Emesis (Syrup of ipecac and Apomorphine). • Gastric lavage (noso-gastric or an oro-gastric tube). • Adsorption by activated charcoal (exceptions poisonings with heavy metals). • Cathartics (hyper-osmotic saline, bulk-forming stimulant, and lubricant laxatives). 3. Enhancement of elimination of absorbed poison. • Forced diuresis (mannitol or furosemide) and pH alteration (↑ degree of the ionization ). • Extracorporeal techniques: • Peritoneal dialysis (Diffusion of toxins from mesenteric capillaries across the peritoneal membrane into dialysate dwelling in the peritoneal cavity). • Hemodialysis (2 catheters are inserted into the patient’s femoral vein. Blood is pumped from one catheter through the dialysis unit (a cellophane bag) and returned through the other catheter. • Hemofiltration (Similar to hemodialysis, except that the blood is pumped through a hemifilter, where waste products and water are removed by hydrostatic pressure. Replacement fluid is added and the blood is returned to the patient). Used for large molecular weight toxicants. • Hemoperfusion (The blood is withdrawn from the patient and passed directly over the adsorbing material contained in sterile columns to remove toxic materials). • Plasmapheresis and Plasma exchange (separation of cellular blood components from plasma then cells are resuspended in fresh frozen plasma and reinfused again). ↑protein binding • Exchange transfusion (removal of the patient’s blood, replacement with fresh whole blood). • Plasma perfusion (combination of plasmapheresis and hemoperfusion).
Principles in management of Poisoned Patient(cont.) Hemodialysis Peritoneal dialysis Semipermeable membrane
Principles in management of Poisoned Patient(cont.) 4. Inactivation of the absorbed poison (Antidotes). • Chelatorsas Deferoxamine, Dimercaprol, EDTA, Penicillamine, DMSAfor HMs. • Cyanide antidoteas Dicobalt Edetate, Cyanide antidote kit (Amylnitrite, Na nitrite, and Na thiosulphate) andHydroxocobolamin. • Calcium saltsas Calcium gluconate and calcium chloride (hydrofluoric acid skin burns, neuromuscular paralysis, ingestion of fluoride salts, calcium channel blocker overdose, B-blocker overdose). I.V. Ca2+ should be given slowly. • Antiveninsagainst spiders and snake bites. • Antidotes to methyl alcohol(10% ethanol), & ethylene glycol(4-methylpyrazole: 4-MP). • 4-aminopyridine (4-AP; ↑ Ca2+ influx), an antagonist of non-depolarizing neuromuscular blocking agents. • Benztropine and diphenhydramine, reverse drug induced dystonias (sustained M.C.) by blocking M receptors and dopamine uptake. • Atropine,antagonizes cholinergic stimuli at muscarinic receptors. • Dantrolene, decreases the release of Ca2+ from the S.R. of skeletal muscle cells. • Flumazenil,competitive inhibitor to benzodiazepine at the GABA-BDZ receptor complex. • Folinic acid (leucovorin) and folic acid, precursor of the active form tetrahydrofolic acid. • Glucagon, Used in the treatment of hypoglycemia or hypoglycemic agent overdoses. • Hyperbaric oxygen,displaces CO from HB, myoglobin and cytochrome oxidase enzyme. Used in CO poisoning, Cyanide and hydrogen sulfide poisoning, CCl4 poisoning. • Methylene blue, an electron carrier used to treat patients who are exposed to methemoglobin forming compounds. • Pyridoxineis essential in the synthesis of GABA within the CNS. It controls isoniazide induced seizures. • Sodium bicarbonate, neutralizes hydrogen ions and raises pH, can reverse QRS prolongation in antidepressant overdose and reverses cardiac conduction defects caused by quinidine-like effects of caridotoxic drugs.
Teratogenesis Teratogenesis is a prenatal toxicity characterized by structural or functional defects in the developing embryo or fetus. It also includes intrauterine growth retardation, death of the embryo or fetus, and transplacental carcinogenesis. Stages of intrauterine human development: • pre-implantation and post-implantation stages (0 8 weeks), teratogenscan kill some of the cells in the blastocyst, resulting in the death of the embryo. • fetal development (9 weeks birth), influence neurologic development, growth, physiologic and biochemical functioning, mental development, and reproductionor death of the fetus. • Drugs that reach the embryo at organogenesis may produce abortion, no effect at all, an anatomic defect, or a metabolic or functional defect that may not be detected until later in life. Thalidomide Syndrome Cleft lip and palate
Teratogenesis; Teratology Education Multifactorial or unknown Genetic 20%-25% 65%-75% Environmental Intrauterine infections 3% Maternal metabolic disorders 4% Environmental chemicals 4% Drugs and medications <1% Ionizing radiation 1%-2%
Teratogenesis (cont.) Dose-effect relationship • Teratogens may demonstrate a dose-effect relationship. • With most agents, a dose threshold for teratogenic effects has not been determined. • Teratogens must reach the developing conceptus in sufficient amounts to cause their effects it depends on its m.wt., polarity, lipid solubility and the existence of a specific protein carrier. FDA Classifications of Drug Risk • No fetal risk shown in controlled human studies in all trimesters. • Animal studies show a risk that is not confirmed in human studies during all trimesters. • Fetal risk shown in controlled animal studies but no controlled human studies are available or studies in humans and animals are not available. • Studies show fetal risk in humans (use of drug may be acceptable even with risks). X. Risk to fetus clearly outweighs any benefits from these drugs. Examples of teratogenic agents • Thalidomide (X).Limb defects and other congenital anomalies • Warfarin (D).Skeletal abnormalities (curvature of the spine) andLimb abnormalities. • Aminoglycosides (C) at high dose. VIII cranial nerve damage. • ACE inhibitors (D).Renal tubular dysplasia, skull and pulmonary hypoplasia. • Antineoplastics (D).Growth retardation, cleft palate, eyes, kidney, cardiac, limbs, skull defects. • Retinoids (X). Heart defect, spontaneous abortion, microtia or cognitive defects. • Other teratogenic agents as Ionizing radiation, infections (virus, syphilis, toxoplasmosis), metabolic imbalance (alcoholism, diabetes, folic acid deficiency, iodine deficiency, hyperthermia, rheumatic and congenital heart diseases.
Prenatal Diagnosis of Teratogenesis • Amniocentesis • 20 ml of amniotic fluid (contains fetal tissues). • Done when a woman is between 14 and 16 weeks pregnant or later. • Able to detected genetic disorders or a chromosomal abnormality. Neural tube defects such as spina bifida can also be detected. • Chorionic villus sampling (CVS) • 30-40 mg of villi cells (have the same genetic makeup as the growing fetus) by transabdominal or transcervical ways. • CVS is usually performed between the 10th and 12th weeks after last menstrual period. • Unlike amniocentesis, CVS cannot detect neural tube defects, such as spina bifida.
Prenatal Diagnosis of Teratogenesis • Biochemical markers • Biochemical markers are used to assess maternal, placental and fetal health. • They help to diagnose and monitor maternal conditions such as gestational diabetes and pre-eclampsia (↑ BP, fluid retention & proteinuria), trophoblastic disease (abnormal trophoblast cells grow inside the uterus after conception) and fetal chromosomal abnormalities. • These biochemical and hormonal tests constitute only one aspect of obstetric care. They should be used together with clinical findings and imaging, particularly ultrasonography.
Mechanisms of Teratogenesis • Interference with nucleic acids:(DNA replication, transcription or RNA translation) • Antimetabolite : methotrexate. • Alkylating agents: Chlorambucil. • Active metabolites of Thalidomide . • Inhibition of enzymes: • Methotrexate inhibits DHFR, thus prevents the formation of folinic acid from folic acid which is essential for embryo growth. • 5-flurouracil inhibits thymidylate synthase leading to inhibition of thymidine monophosphate (dTMP) synthesis, inhibition of DNA synthesis. • Glucose-6-phosphate dehydrogenase inhibitors (6-aminonicotinamide) decrease energy production in cells (such as erythrocytes).
Mechanisms of Teratogenesis (cont.) • Deficiency of energy supply needed to build organs: • Glucose deficiency • Deficiency of glucose in diet, • G-6-PD inhibitors (6-aminonicotinamide) interfere with glycolysis, • Drugs affecting Kreb’s cycle (the pesticide fluroacetate). • Interference with O2 supply or utilization. E.g. CN toxicity (cytochrome oxidase inhibitor). • Hypoxia: CO toxicity (decrease in both O2 delivery + osmotic pressure to fetus) as in phenytoin toxicity. This can induce edema and hematomas, which in turn can cause mechanical distortion and tissue ischemia. • 4. Lack of substrates: • Decrease of vitamins or minerals intake as Zinc. • Failure of absorption from GIT as in GIT infection e.g. diarrhea or bile acid deficiency. • 5. Osmolar imbalance. • E.g: ethylenethiourea exposure causing lower osmolality of exocoelomic fluid (ECF) surrounding the embryo that causes water to move out of the ECF. ECF will accumulate in the embryo which leads to localized edema in the embryo resulted in inhibition of growth/differentiation and increased incidences of malformations.
Mechanisms of Teratogenesis (cont.) 6. Mutationsare heritable changes in the genome of a cell or an organism. • There are three different levels at which mutation takes place, namely at the DNA sequence level (gene mutations), at the chromatin structure level (structural chromosome aberrations) and at the chromosome number level (numerical chromosome aberrations). • Induced somatic cell mutations the development of secondary tumours. • Induced germ cell mutations abnormal reproductive outcomes. • Gene Mutations • Changes in base pair sequence within a gene. • Polymorphism; are variation in the DNA sequences. • Can alter the amino acid sequence of the protein encoded by the gene. • Arise either through the base substitutions, or deletion or insertion (frameshift) of one or more bases from one or more codons, leading to a mispairing in the replication & transcription.
Mutations: Gene Mutations (cont.) • The consequences of gene mutations can be: • Missense mutation : the code of an amino acid is altered into the code of another amino acid (expressed as decreases in function rather than by total loss). • Nonsense mutation : the code of an amino acid is changed into a termination code (causing a premature transcription termination and a shortened protein). • Most of these mutations lead to missing gene products or products that are unable to function. In rare cases, however, a mutation can also bring about the synthesis of a "better" protein, i.e., one that is better suited for the environmental conditions. • EeroMantyranta, a Finnish cross-country skier who won two gold medals in the 1964 Olympics, was born with a mutation in the erythropoietin receptor gene that allows his blood to carry significantly more oxygen than the average person's. Eero Mantyranta
Detection of Gene mutation Single gene defects can be diagnosed using nucleic acid analyses, e.g.;
Examples of Gene Mutations (Autosomal dominant inheritance,50%) • Marfan's syndrome (abnormalities in connective tissues) due to mutations in the FBN1 gene on 15q21.1, which encodes fibrillin-1, a glycoprotein component of the extracellular matrix. • Aniridia (incomplete formation of the iris) due to mutations in the PAX6 gene on 11p13. • von Recklinghausen's disease (Neurofibromatosis: changes in skin coloring and the growth of tumors along nerves in the skin, brain, and other parts of the body) due to mutations in the neurofibromin gene on chromosome 17, that is responsible for control of cell division.
Examples of Gene Mutations (Autosomal recessive inheritance,25%) • Cystic fibrosis (disease of the mucus glands) due to mutations in the CFTR gene on 7q31.2. • Hemo-chromatosis (accumulates excess iron) due to mutations in the HFe gene on chromosome 6 at location 6p21.3. • Sickle cell anemia (atypical hemoglobin S) due to mutations in the β-globin chain of haemoglobin, which results in glutamic acid being substituted by valine at position 6. The β-globin gene is found on chromosome 11, more specifically 11p15.
Examples of Gene Mutations (X chromosomal inheritance) • Duchenne's muscular dystrophy due to mutations in the gene DMD, in Xp21. The DMD gene codes for the protein dystrophin, an important structural component within muscle tissue. (muscle weakness → paralysis) • Hemophilia A and B (deficiencies of clotting factor VIII and factor IX, respectively). Hemophilia B is caused by Variants (mutations) in the F9 gene which codes for coagulation factor IX.
Examples of Gene Mutations (X chromosomal inheritance (cont.) 3. Red-green blindness. The two genes in which mutation is associated with red-green color vision defects are OPN1LW (opsin 1 long wave), encoding the red pigment and OPN1MW (opsin 1 middle wave), encoding the green pigments. • 74 (normal color vision) • 21 (dichromacy or anomalous trichromacy) • No numbers (achromatopsia) • 37 (normal color vision) • No numbers (protanopic) • 56 (normal color vision) • No numbers (tritanopic) • 49 (normal color vision) • No numbers (deuteranopic)
Mutations: Structural Chromosome Aberrations • Structural Chromosome Aberrations are changes in chromosome structure and involve gross alteration of the genetic material and are detected by light microscopy. • Structural aberrations are the result of chromosomal breaks that occur during cell division. Here deletion, rings and duplication (unstable) lead to an abnormal phenotype, while inversion,insertion as well as translocation (stable) can be balanced. This means that the carrier of this structural aberration can escape notice phenotypically, because the entire genetic material is present.
Examples of Structural Chromosome Aberrations Cri du chat syndrome (cry of the cat) due to the deletion of part of the short arm of chromosome 5. Wolf-Hirshchhorn syndrome (mental and growth retardation) is due to the partial deletion of part of the short arm of chromosome 4. CATCH 22 syndrome (cardiac, abnomal faces, thymic hypoplasia, cleft palate, hypocalcemia)is due to the deletion of the q11.13 region on chromosome 22.
Mutations: Structural Chromosome Aberrations(cont.) Many of Structural Chromosome Aberrations can be detected with staining techniques such as Banding techniques. • In this karyogram ring formations of chromosomes 1, 7 & 15 can be seen. • Karyogram of the baby demonstrating deletion in chromosome 7 (arrow). Fluorescence in situ hybridization (FISH) techniques • 2 translocations between chromosomes 1 and 8. • Translocation between chromosomes 3 and 21. • Aberrant chromosome 14 with an additional part derived from the same chromosome on the short arm. • Trisomy of chromosome 13 was identified.
Mutations: Numerical Chromosome Aberrations (cont.) • These are changes in the number of chromosomes in the genome. • When mutations change the number of whole chromosome sets present, polyploid cells result. • When mutations change parts of chromosome sets, aneuploid cells result. • The normal diploid genome is euploid, and contains a complete set of chromosomes from each parent, e.g. 2n = 46 for humans. • Thus, 45 or 47 chromosomes would be described as aneuploid, whereas cells with 69 chromosomes would be described as triploid (3n). • Aneuploid nomenclature for autosomes in diploid organisms:The aneuploid condition 2n-1 is called monosomic (meaning “one chromosome loss”),2n+1 is called trisomic, and 2n-2 (where the -2 represents homologs) is nullisomic. • Aneuploid nomenclature for sex-chromosome in diploid organisms: The symbolism simply lists the copies of each sex chromosome, such as XXY, XYY, XXX, or XO.
Examples of Numerical Chromosome Aberrations • Down’s syndrome (47, Y-21-21)
Examples of Numerical Chromosome Aberrations (cont.) Klinefelter’s syndrome (47, X-X-Y)
Examples of Numerical Chromosome Aberrations (cont.) Turner's syndrome (45, X-O)