Understanding Thyroid Disorders: A Comprehensive Guide
Explore the functions, disorders, and management of the thyroid gland with detailed information on congenital and acquired hypothyroidism. Learn about the impacts and outcomes of thyroid disorders for effective diagnosis and treatment.

Understanding Thyroid Disorders: A Comprehensive Guide
E N D
Presentation Transcript
Thyroid gland • Thyroid gland is composed of over a million cluster of follicles • Follicles are spherical & consists of epithelial cells surrounding a central mass (colloid) • Thyroglobulin is a storage room • Two main hormones: – Tetraiodothyronine (Thyroxin) = T4 – Triiodothyronine = T3
Production of Thyroid Hormones NIS (Na+/I- Sympoter) TPO
t1/2 = 5-7d t1/2 = < 24 hrs
Effects of thyroid hormones • Foetal brain & skeletal maturation • • Increase in basal metabolic rate • • Inotropic & chronotropic effects on heart • • Increases sensitivity to catecholamines • • Stimulates gut motility • • Increases bone turnover • • Increase in serum glucose • Decrease in serum cholesterol • • Conversion of carotene to vitamin A • • Play role in thermal regulation
Thyroid disorders: Aetiology • Congenital • Acquired • – Primary • – Secondary • – Tertiary
Congenital hypothyroidism • Agenesis (No goiter) or dysgenesis (aplasia, hypoplasia, ectopic gland) are the commonest causes…..85% • Dyshormonogenesis (10%) and a goiter will be present. Pendred syndrome with sensorineural deafness is the commonest (often euthyroid). • Transplacental maternal TSH receptor blocking Abs (TRBAb) account for 5% of cases. • Pituitary failure and maternal ingestion of goitrogens are other causes
Congenital hypothyroidism • One of the most common treatable causes of Mental retardation • CH Screening is the most cost effective program • Almost all affected Newborns have no S/S at birth • Congenital Anomalies increased by 10%(cardiac) • It is permanent in more than 90% of the cases • The earlier the diagnosis the better is the IQ
A. Delayed epiphyseal appearance B. epiphyseal dysgensis
Signs of congenital hypothyroidism •31% prolonged jaundice • 23% umbilical hernia • 21% constipation • 21% macroglossia • 19% feeding problems • 16% hypotonia • 16% hoarse cry • 13% large posterior fontanelle • 10% dry skin • 5% hypothermia • 2% goiter • 40% delayed bone age
Diagnosis • Congenital hypothyroidism • • Thyroid hormone level • • TSH • • Thyroid scan • Maternal investigations: TFT and Abs • Acquired Hypothyroidism • • TSH • • fT4 • • Thyroid antibodies • • Thyroid ultrasound • • TSH: low in secondary hypothyroidism -high in primary hypothyroidism • • TRH test: to differentiate between secondary & Tertiary hypothyroidism
Management of congenital hypothyroidism • Documentation • – Free T4, TSH • • Thyroid scan, ultrasound (optional) • • Treatment (normal size full term) • – start L-thyroxin at 10-15 mcg/Kg daily • – Monitor TSH every 2-3 months during first 2 • years of life.
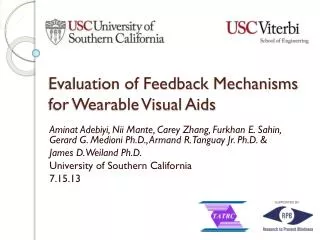
A 15 years old female with classic Graves disease
HOW therapy can make a difference Prior to Therapy 7 months after therapy
Question • A 13 year-old diagnosed with congenital hypothyroidism was brought in by mother after missing appointments for >1 yr. Physical examination reveals length at the 5th percentile, weight at the 10th percentile, dry skin, and non pitting edema in bilateral lower extremities. Mother also concerned with constipation. You ordered TSH and FT4 and increased the thyroid hormone replacement therapy from 50mcg to 100mcg.
Question Of the following, the MOST likely long-term outcome in this child: • Adrenal Insufficiency • Diabetes mellitus • Learning disorder • Normal adult height • Precocious puberty
Answer - C • Children who have severe hypothyroidism at birth tend to have poorer intellectual outcomes than their siblings, even if therapy is started in the first few days after birth • With continued and appropriate thyroid hormone therapy, this child should grow normally in height, and adult height should be appropriate for the family. However, this child has been chronically undertreated for many months. • Congenital hypothyroidism is not associated with adrenal insufficiency, • Precocious puberty is not an outcome of congenital hypothyroidism unless a child is overtreated with thyroid hormone and develops premature maturation, which is very unusual. Some children who have severe acquired hypothyroidism have manifested signs of sexual precocity that disappear after treatment of the hypothyroidism (Van Wyk-Grumbach syndrome).
CH • Thyroid dysfunction in the neonate can be broken down into hypothyroidism and hyperthyroidism. Transient versus Permanent dysfunction. • Transient hypothyroidism is defined by low thyroxine (T4) and elevated TSH concentrations that ultimately return to normal.Secondary to iodine deficiency, excess maternal anti-thyroid drugs reaching the foetus in utero, and transplacental passage of maternal thyrotropin receptor-blocking antibodies. • In North America, transient hypothyroidism is rare, about 1 in 50,000, but is increased in countries with iodine deficiency. It also appears to be increased in preterm infants as compared to term infants. • Thyroid dysgenesis (1:4,000) accounts for about 85% of primary congenital hypothyroidism, due to an ectopic thyroid gland, or thyroid aplasia and hypoplastic thyroid.Others due to dyshormonogenesis (1:40,000).
CH • Even rarer causes of primary hypothyroidism include errors in metabolism and transport of thyroid hormone, and defects in the thyroid hormone receptor. • The most common cause of secondary hypothyroidism is hypopituitarism (1:100,000). • Newborn screening has greatly aided in the prompt diagnosis of congenital hypothyroidism. If an infant is found to have an abnormal newborn screen, they should be immediately referred to a pediatric endocrinologist, as the goal is to treat as soon as possible due to the known importance of thyroid hormone on brain development.
Adrenal disorders CONGENITAL ADRENAL HYPERPLASIA (CAH)
Basic anatomy of the human adrenal gland Length: 4 – 6 cm; Width: 2 – 3 cm. Weight : 3 – 5 g each
Without cortisol, we could not live • Cortisol functions: • help the body respond to stress • helps maintain blood pressure and cardiovascular function • helps slow the immune system's inflammatory response • helps balance the effects of insulin in breaking down sugar for energy • helps regulate the metabolism of proteins, carbohydrates, and fats • helps maintain proper arousal and sense of well-being • Pituitary gland, (at base of brain) makes ACTH that drives the adrenal gland • production of glucocorticoids
Adrenal insufficiency • Primary or secondary • Congenital or Acquired (for each) • Symptoms • Weight loss • Anorexia • Weakness • Fever • Depression • Nausea / abdo pain • Myalgia • Confusion • If due to CAH: Hypoglycaemia, Dehydration and Hypotension – over virilization (due to excess of sex steroids)