Download
1 / 53
550 likes | 713 Vues
Evaluation of Hip Pain in Runners. John Hill, DO,FACSM, FAAFP. University of Colorado Director of Primary Care Sports Medicine Fellowship Saturday, May 17, 2014. Objectives At the completion of this activity , you will be able to:. Better perform a focused hip examination

E N D
Evaluation of Hip Pain in Runners John Hill, DO,FACSM, FAAFP University of Colorado Director of Primary Care Sports Medicine Fellowship Saturday, May 17, 2014
ObjectivesAt the completion of this activity, you will be able to: • Better perform a focused hip examination • Recognize and manage improper running biomechanics to prevent injuries • Discuss how core stability impacts many running injuries • Apply these principles to return the “athlete” back to running
ObjectivesIn addition to the previous objectives… • You will understand that running is not evil • Most of us were born to run!
Disclosure Statement • Newton Shoes: Physician Advisory Board • MuscleSound: Physician advisor for software development to determine muscle glycogen content using Ultrasound.
Leadville Trail 100 • After running more than 28 hours, I am still smiling, why…. • I finally learned what I am going to teach you
It is all about Biomechanics Tarahumara runner Arnulfo Quimare and Ultra-running legend Scott Jurek
It is all about Biomechanics Flexed at the waist Heel strike Over striding Low arm position Hip drops with each step Knee collapses in valgus No smile on his face, this dude is suffering
copes with impact and takeoff --extends from spine to foot
Foot strike • Support • Take-off • Swing swing takeoff foot strike support
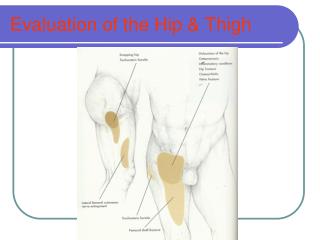
Differential Diagnosis of Running Injuries • Intra-articular • Chondral • Labral • Capsular • Extra-articular • Systemic
Snapping hip ITB tendinitis Bursitis Flexor tendinosis SI joint pain Hamstring strain Soft tissue impingement Iliopsoas Athletic pubalgia Hernia Adductor tendinosis Extra-articular
What about Kids? • Developmental Dysplasia of the Hip • Legg Calve Perthes Disease • Slipped Capital Epiphysis • Previous Trauma
Hip Scan • History: symptom response • Functional Movement Screen • Weight Bearing tests • AROM • PROM with over pressure – Flexion/Abduction • Manual muscle testing • Distraction/Compression with movement • Ligament evaluation • Marching test for sacroiliac movement • FABER
Exam: ROM • Active/Passive: • Flexion (110-120’) • Extension (10-15’) • Abduction (30-50’) • Adduction (30’) • Internal Rotation (0-50’) sup/prone • External Rotation (30-90’) sup/prone
Exam: Strength Testing • Flexion: • Psoas, Iliacus, rectus femoris, sartorius, pectineus, adductor long/brev, gracilis • Extension: • Biceps femoris, semimembranosus, semitendinosus, glut max, glut med (posterior part), adductor magnus (ischiocondylar part) • Adduction: • Adductor longus, adductor brevis, adductor magnus, gracilis, pectineus
Exam: Strength Testing • Abduction: • Tensor fascia latae, glut minimus, glut medius, glut maximus, sartorius • Internal Rotation: • Adductor long/brev/magnus, Glut med (anterior part), glut minimus (anterior part), tensor fascia latae, pectineus, gracilis. • External Rotation • Glut max, obturator int/ext, quadratus femoris, piriformis, gemellus sup/inf, sartorius, glut med (posterior part)
FADIR Test Flexion / Adduction / IR Impingement test (positive)
FABER Test Flexion / Abduction / ER
Exam: Special Tests • Gluteus Medius Strength Test • Gluteus Maximus Strength Test • Adductor Testing • Piriformis Test • + if pain with stretching piriformis muscle • Fulcrum Test • + if pain is elicited • Site of pain is usually near site of stress fracture
Core stability First recognized importance in late 1980s and early 1990s General population: multiple exercise programs and equipment focused on core stability and benefits of improving stability
Core stability First recognized importance in late 1980s and early 1990s General population: multiple exercise programs and equipment focused on core stability and benefits of improving stability Does this apply to runners?
Definition No universally accepted definition of core stability Kibler: “The ability to control the position and motion of the trunk over the pelvis to allow optimum production, transfer, and control of force and motion to the terminal segment in integrated kinetic chain activities”
Definition of the core Includes the spine, hips, pelvis, proximal lower limbs, and abdominal region
Definition of the core Diaphragm Paraspinals and Gluteals Abdominals Pelvic Floor and Hip Girdle Musculature
Definition of the Core • Strength of the core muscles: • Allows the system to mechanically stabilize the spine then distribute and deliver compressive, translational, and shear forces to and from the rest of the body
Theory of Plyometrics • Plyometric training: • Involves exercises in which the active muscles are stretched prior to shortening • Usually requires explosive strength training • Invokes specific neural adaptations (ie, increased activation of motor units) • Less muscle hypertrophy than static strength training • Running is a plyometric activity
Theory of integration • Rehab from injuries: • Benefits from strength exercises • Benefits from plyometric training • Integration of the two improves your results
Theory of integration • Return to running after an injury: • Must be able to demonstrate competence with plyometric exercise (proper running form) • To perform plyometric exercises safely, must increase core stability with static load strength training
Core stability: the evidence Prevention of injury Treatment of injuries Effect on performance
Prevention of injury— does static core weakness predispose to injury? Back pain: delays in trunk motor control reflex are predisposing factor (Cholewicki, 2005) Patellofemoral pain: weakness in the gluteus medius predisposes to PFS (Willson, 2011) Hamstring injuries: early fatigue in abdominal muscles likely a contributor (Devlin, 2000) Knee Ligament injury: increased trunk displacement and decreased proprioception on testing predicted knee ligament injury for females, not males (Zazulak, 2007)
Evaluating core strength in Runners Wide variety of movements associated with sports need sufficient strength in hip and trunk muscles in all three planes of motion Contribution of specific muscles depends on direction and magnitude of trunk loading (Cholewicki 2002)
Evaluating core strength • Athletes may have good core strength when tested by low exertion exams • Need to do more functional testing • Remember, this person is not just walking around the house and going to the grocery store
Evaluating core strength • 3 tests • 1. Pelvic alignment • 2. Single leg squat and hop test • 3. Side plank with side leg raise
Good pelvic alignment: horizontal waist Poor pelvic Alignment: forward pelvic tilt
Evaluating core strength • Pelvic tilt • Forward tilt: often see weakness in quadratus lumborum, rectus abdominis, and obliques
Evaluating core strength • Single Leg Squat • Global core stability • Should see alignment maintained between hip, knee, and ankle • Watch for contralateral hip dropping and knee moving into valgus • If single leg squat performed competently, move on to lateral step down test
Single leg squat Good limb alignment Single leg squat Valgus collapse of knee Single leg side step Good limb alignment
Evaluating core strength • Hop test • Similar to single leg squat, more dynamic • Requires neuromuscular control, core strength and stability • Evaluate knee alignment, height of jump, and stable, aligned soft landing
Evaluating core strength • Side plank • Both sides • Measures lateral core strength—Quadratus lumborum • Examiner notes how long patient can hold position • Ideal length of holding: 45-60 seconds
Evaluating core strength Side plank
Evaluating core strength • Side leg raise • No trunk flexion • Upper leg abducted completely with maximal hip external rotation (toe pointed to ceiling) • Fully recruits gluteus medius • Examiner resists motion and evaluates strength
Evaluating core strength Side leg raise
Evaluating core strength • Combining exercises • If proficient with both side plank and side leg raise combine these exercises • Assess neuromuscular coordination, hip adductor strength, and abnormal recruitment of the iliopsoas • Weak abductors recruit iliopsoas and see forward flexion at waist • Goal to perform 30 on each side
Evaluating core strength Combined side plank and side leg raise
Evaluating core strength Clinicians should not assume athletes are more competent with dynamic core stability than the general population Dynamic testing can unmask subtle deficiencies
Restoring function by addressing core deficiencies Important to achieve adequate static core strength prior to pushing dynamic, plyometric rehab Often therapist or athlete will push dynamic plyometric rehab too soon re-injury Need at least 3 sets of 15 with combined activity to progress to plyometric rehab
Maintenance of core stability Important to maintain once athlete returned to sport Continue 3 sets of 30 of the combined side plank and side leg raise on each side, 3 days per week