The Shoulder
The Shoulder . David Limb Consultant Orthopaedic Surgeon Leeds Teaching Hospitals. Anatomy Variations of normal What happens with age Common problems. Arm is connected to body via the shoulder blade and collarbone Humerus then forms a joint with the shoulder blade

The Shoulder
E N D
Presentation Transcript
The Shoulder David Limb Consultant Orthopaedic Surgeon Leeds Teaching Hospitals
Anatomy • Variations of normal • What happens with age • Common problems
Arm is connected to body via • the shoulder blade and collarbone • Humerus then forms a joint with the • shoulder blade • Shoulder movement involves • the joint between the collarbone and chest • the joint between collarbone and shoulder blade • the ‘joint’ between shoulder blade and chest • the joint between humerus and shoulder blade
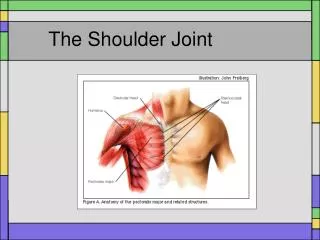
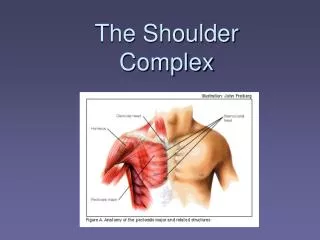
Shoulder blade is suspended by muscles 26 muscles cross the shoulder joint
‘shoulder’ joint unusual – socket is mostly soft tissues • Trade off of stability to allow maximum mobility
Cuff Deltoid Shoulder movement involves balanced couples
Clinical examination good enough to direct non-operative treatment Often need imaging before surgical treatment
Investigations Ultrasound
MRI Arthroscopy
Problems - Impingement • Arthroscopic subacromial decompression • 700% increase in UK over last 10 years • Paracetamol for the shoulder headache
Rotator cuff ‘tears’ • Prevalence • about 50% in their 50’s have partial tears • about 1 in 3 in 70’s have full thickness tears • about 50% in 80’s have complete tears
Rotator cuff repair with tissue anchors • can be carried out arthroscopic or open • anchors can be metallic or absorbable plastics • 80% success rate in terms of pain relief and restoration of function • Rehabilitation to heavy use is 6 months • Up to 50% ‘fail’ within the first six months
Posterior dislocation ‘commonly’ missed
Arthroscopic stabilisation • employs suture anchors • metallic or absorbable • success rates catching up with open surgery
Shoulder injections • Steroid can cause painful reaction for several days • Infection can first manifest as pain • Fortunately infection extremely rare • Adjunct to nonoperative treatment • May inhibit healing of surgically repaired cuff tears
Shoulder prostheses Now well established in the treatment of shoulder arthritis and fractures Survivorship comparable to hip and knee replacement
Do we have the evidence? In 2010 2 of largest grants ever were awarded in orthopaedics Health technology assessment grants – Dept of Health £2m – What is the place of surgery in rotator cuff disease £1m – What is the place of surgery in managing shoulder fractures
Summary • In the normal shoulder there is a trade off of stability for mobility • There is a wide range of ‘normal’, even the anatomy • Very significant degenerative lesions occur with age • There is a very wide spectrum of outcome after treatment ?