Download
1 / 99
1k likes | 1.41k Vues
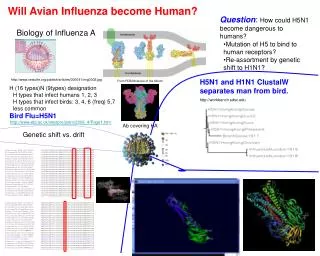
Management of Suspect Cases of Human Infection with Avian Influenza A (H5N1) Virus. Outline. Part 1: Background and epidemiology of avian influenza A (H5N1) virus infection in humans Human H5N1 clusters Clinical features of human infection with H5N1 virus Part 2:

E N D
Management of Suspect Cases of Human Infection with Avian Influenza A (H5N1) Virus
Outline • Part 1: • Background and epidemiology of avian influenza A (H5N1) virus infection in humans • Human H5N1 clusters • Clinical features of human infection with H5N1 virus • Part 2: • Assessing case patients: Collecting clinical and epidemiologic information • Specimen collection and diagnostics • Treatment
Management of Suspect Cases of Human Infection with Avian Influenza A (H5N1) Virus Part 1: Epidemiology and Clinical Features 3
Part 1: Learning Objectives • Understand the epidemiology of known human H5N1 cases and risk factors • Importance of clusters • Recognize clinical features of H5N1 in humans
Epidemiology of Influenza A(H5N1) Virus Infection of Humans Photo: T. Uyeki, CDC
Global Epidemiology • 409 cases have been reported to WHO from 15 countries* • Case fatality proportion = 256/409: ~ 63% • Human surveillance has focused upon severe respiratory disease (pneumonia) *Reported as of March 2, 2009
Human Avian Influenza A (H5N1) Cases by Onset Date and Country(as of 23 November 2009) As of 23 March 2009, total of 412 cases were reported officially to WHO * Cases missing onset date are excluded: 1 Viet Nam, 13 Indonesia, 3 Azerbaijan, 20 Egypt, 1 Turkey, 1 Iraq, 1 Nigeria ** CFR Trend: computed based on cumulative dead & total number of cases
WHO Summary of H5N1 cases • Epidemiologic summary of H5N1* • Median age: 18 years (range 3 months - 75 years) • 90% of cases were aged <40 years • Male to female ratio = 1:1 • Median time to hospitalization: 4 days • Case fatality proportion: ~60% • Highest case fatality: 10-19 years (76%) • Lowest case fatality: ≥50 years (40%) • Median time to death: 9 days (range 2 – 31 days) *Update: WHO-confirmed human cases of avian influenza A(H5N1) infection, November 2003–May 2008. Weekly Epidemiological Record, NO. 46, 14 November, 2008 WHO Avian Influenza http://www.who.int/csr/disease/avian_influenza/en/
Review Question 1 Which two countries have reported the most cases Influenza A (H5N1) to WHO to date? a. Indonesia and Vietnam b. Egypt and Thailand c. China and Cambodia d. India and China Answer: a. Indonesia and Vietnam
Review Question 2 What age group has the highest reported case fatality rate from H5N1 virus infection? a. 0-9 years old b. 10-19 years old c. 20-29 years old d. > 50 years old Answer: 10 – 19 years old
Risk Factors: Exposures in the Week Before Illness • Touching sick or dead poultry • Slaughtering, preparing for cooking • Touching dead wild birds • Having sick or dead poultry in the household • Visiting a live poultry market Photo: AP/ Bikas Das
Risk Factors: Culture-Specific Risk • Eating uncooked duck blood • Defeathering of swans • Playing with dead chickens • Contact with roosters used in cock fighting Photo: TIME Magazine / John Stanmeyer
Avian to Human Transmission of H5N1 • Primary mode of transmission is avian-to-human (zoonotic): • Exposure to infected poultry • Preparing or consuming uncooked or undercooked H5N1 virus-infected poultry or poultry products • Indirect transmission may occur through: • Inhalation of aerosolized H5N1 virus infected material • Contact with surfaces contaminated with infected poultry feces • Contact with infected animals that ate dead poultry
Human-to-Human Transmission of H5N1 Virus Infection • Probable but limited, non-sustained* human-to-human transmission • Very rare, but documented • Occurred during close, prolonged, unprotected contact with a human H5N1 case • Mostly in family members • Transmission in hospital setting reported *Currently, no evidence of sustained human-to-human H5N1 virus transmission
Occurrence of H5N1 Clusters • >25% of all cases have occurred in clusters • Clusters are 2 or more H5N1 cases that are epidemiologically-linked • Occurred in several countries • Hong Kong (2003) • Thailand (2004) • Indonesia (2006)
Human Case Cluster, Hong Kong 2003 Family of five Hong Kong residents visited Fujian Province, southern China in late January 2003 7-year old girl developed pneumonia and died, was buried, but not tested Four survivors returned to Hong Kong Father and son were hospitalized with pneumonia; both confirmed with H5N1, father died No direct link between cases and avian flu infection in poultry was found
Human Case Cluster, Thailand 2004 11-year old girl who lived in a rural village with her aunt where poultry deaths occurred Mother lived near Bangkok (no poultry exposure) The girl developed fever and lower respiratory tract disease, hospitalized with pneumonia Mother and aunt traveled to hospital to provide care The girl died 24 hours later Mother and aunt became sick, were confirmed with H5N1 virus infection; mother died Probable human-to-human transmission of H5N1 virus from girl to her mother and aunt
Human Case Cluster, Indonesia 2006 A large H5N1 family cluster occurred in North Sumatra 1 probable + 7 confirmed H5N1 cases 7 deaths H5N1 virus was isolated from 7 cases Index case was likely infected by contact with sick/dead chickens Limited human-to-human-to-human transmission
Interpretation of Case Clusters Cases with similar illness onset dates Same exposure source, similar incubation period? Cases with illness onset separated in time Similar exposure source, different incubation periods? Different exposure sources? Limited human-to-human transmission?
Significance of Case Clusters Increase in number and size of clusters, or increase in number of mild cases can indicate: That H5N1 viruses are spreading to more people Possible increased adaptability of H5N1 viruses to humans Signal for: An increased pandemic threat and a change in WHO Pandemic Alert Period Phases The beginning of a pandemic Early containment measures
Assessing for Possible Human-to- Human H5N1 Virus Transmission • Documented exposure to a confirmed, probable, or suspected human H5N1 case, • AND • The time interval between contact with a suspected, probable, or confirmed H5N1 case and illness onset is 7 days or less, • AND • No other sources of H5N1 exposures • Such as: birds, other animals, feathers, droppings, fertilizers made of fresh bird droppings, live poultry markets, contaminated environments, or laboratory specimens
H5N1 Cluster Summary • ~25% of confirmed H5N1 cases have occurred in clusters worldwide • Mostly among blood related family members • Most cluster cases had contact with sick birds • Evidence of limited, non-sustained, human-to-human contact has occurred • Clinically mild pediatric H5N1 cases identified during investigations of severely ill index cases • Changes in size, number or epidemiology of clusters could signal important viral changes/adaptability, or pandemic • Epidemiologic evidence that H5N1 virus can be transmitted from patients to healthcare workers
Review Question 3 If you recognize a cluster of human H5N1 cases, what would cause you to suspect that human-to-human transmission of H5N1 virus has occurred? • Documented exposure to a confirmed, probable, or suspected human H5N1 case • The time interval between contact with a suspected, probable, or confirmed H5N1 case and illness onset is 7 days or less • No other apparent source of H5N1 exposure • 3 or more cases are reported • H5N1 is isolated from common environment of cases Answer: a,b, and c
H5N1 Viral Infection in Humans • Incubation period • Generally from 2 to 7 days • Viral shedding period for H5N1 virus • Still largely unknown • May be 2 weeks or longer • Longer for children and immune compromised
H5N1 Clinical Manifestations • Common signs and symptoms: • Fever ≥38C, cough, shortness of breath, difficulty breathing • Other findings (less common): • Sore throat, headache, muscle aches, diarrhea • Clinical findings are non-specific, and are similar to other common acute respiratory diseases • Critical to ask about H5N1 exposures
Possible Complications of H5N1 Infection • Most common: pneumonia • May progresses to respiratory failure • May requires mechanical ventilation • Acute respiratory distress syndrome (ARDS) • Gastrointestinal disease • Multi-organ failure • Heart and kidney dysfunction • Neurologic symptoms • Encephalitis, seizures, altered mental status, progression to coma
H5N1 Pathogenesis High H5N1 viral levels are associated with an abnormal inflammatory response Other blood changes Decreased white blood cell count Low lymphocyte count Mild to moderately decreased platelet count Infection and inflammation contribute to respiratory failure and multi-organ failure Cytokine dysregulation (cytokine “storm”) 30
Review Question 4 What clinical signs and symptoms are pathognomonic (distinguishing) for Influenza A (H5N1) infection? • Fever • Cough • Shortness of breath • Sore throat • Pneumonia • Gastrointestinal symptoms • None of the above Answer: g. These symptoms may typically occur, but they are non-specific and similar to other acute respiratory diseases.
Part 1 Summary: Epidemiology • Most human H5N1 cases have been healthy children and young adults • Epidemiology and exposure sources critical to suspecting a case • Most H5N1 cases had direct contact with sick or dead poultry or birds in the week prior to illness onset • Limited, non-sustained human-to-human transmission of H5N1 virus is rare, but has occurred
Part 1 Summary: Clinical Manifestation • Signs and symptoms of H5N1 infection are non-specific and are observed in other respiratory diseases: • Fever, cough, shortness of breath, difficulty breathing • Pneumonia • Peripheral blood changes may occur but are non-specific
Management of Suspect Cases of Human Infection with Avian Influenza A (H5N1) Virus Part 2: Diagnosis, Management, and Treatment
Part 2: Overview • Clinically assessing suspected patients: Collecting clinical and epidemiologic information • Diagnostic and laboratory tests • Current recommendations for clinical treatment
Part 2: Learning Objectives • Identify important sources of clinical and epidemiologic information • Recognize laboratory tests used for identification of new cases • Clinical specimen collection, diagnostic and laboratory tests • Know the treatments and interventions for suspected case-patients and their contacts
Part 2: Learning Objectives, cont • Know what pharmaceutical treatments are available for seasonal and pandemic influenza • Understand the difference in the recommendations between seasonal vs. pandemic flu treatment
Assessing Suspected H5N1 Patients Does the patient have findings consistent with H5N1 virus infection? • Collect clinical history and data on clinical findings • Evaluate epidemiological data • Consider clinical, laboratory, and epidemiologic information together
Clinical Data to Collect • Date of illness onset • Signs and symptoms • Routine laboratory results • Complications • Type and date of onset • Clinical specimens collected for H5N1 testing • Precautions used, breaks in precautions
Clinical Data • Common signs and symptoms: • Fever • Cough • Shortness of breath • Difficulty breathing • Other signs and symptoms that may occur: • Sore throat • Sputum production (may be bloody) • Diarrhea / abdominal pain • Muscle aches • Headache • Runny nose
Clinical Complications • Respiratory failure • Complication from pneumonia within a few days to 2 weeks after illness onset • Acute Respiratory Distress Syndrome • Multiple organ failure • Renal dysfunction • Cardiac dysfunction • Abnormal lab values • Low lymphocytes: <1500 / mm3 • Low platelets: < 150,000 / mm3 • Normal lymphocyte count • 1500 - 4000 / mm3 • Normal platelet count • 150,000 - 400,000 / mm3
Medical Charts Include: • Demographic information • Medical history • Illness signs and symptoms • Physical examination findings • Treatment • Laboratory testing results
Epidemiologic Context Potential exposure to H5N1 • Occupational exposure • Animal culler, veterinarian, health care workers • Residence or travel in area affected by H5N1 outbreaks in birds or animals (e.g., poultry market) • Direct contact with dead or diseased birds or other animals in affected area • Close contact with a person with H5N1 virus infection, unexplained moderate or severe acute respiratory illness Warning!Even if NO reports of ill poultry in a location, there could be disease in that area, especially if poultry influenza vaccines are used or reporting is poor
Sample Patient Chart:Exposure History Contact with ill people? (If yes, date and name, relationship to patient) ___________________________________________ ___________________________________________ Contact with diseased poultry (Live or dead)? (If yes, date and location) ___________________________________________ ___________________________________________ Recent travel? (If yes, date and location) ___________________________________________ ___________________________________________ Other close patient contacts (Household members, close coworkers) ___________________________________________ Are any of these contacts ill?
Review Question 5 What are the critical pieces of epidemiologic information that must be collected from a patient with illness that is clinically compatible with Influenza A (H5N1) infection? Answer: • Occupational exposure - Animal culler, veterinarian, health care workers • Residence or travel in area affected by H5N1 outbreaks in birds or animals (e.g., poultry market) • Direct contact with dead or diseased birds or other animals in affected area • Close contact with a person with H5N1 virus infection, unexplained moderate or severe acute respiratory illness
Use All Information • Clinical signs compatible with H5N1 virus infection • History suggests exposure to H5N1 virus 7 days prior to symptom onset • Are there multiple cases or respiratory deaths in the same family or in contacts? • Send samples for laboratory confirmation
Diagnostic and Laboratory TestingSuspected Human H5N1 Case Clinical specimen collection Diagnostic tests Laboratory testing Imaging Chest X-ray 49
Clinical Specimens: Lower Respiratory Tract H5N1 viruses primarily infect lower respiratory tract tissue Deep lung tissues Best specimens for detecting H5N1 viruses: Lower respiratory tract Endotracheal aspirates from intubated, mechanically ventilated patients Bronchioalveolar lavage (BAL) 50