Bladder Diverticuli
Bladder Diverticuli. May be congenital Usually secondary to chronic obstruction of bladder outflow. There will be urinary stasis: - infection. - stone formation. - tumor. Readily seen on all imaging , may deform the adjacent bladder or ureter.

Bladder Diverticuli
E N D
Presentation Transcript
Bladder Diverticuli • May be congenital • Usually secondary to chronic obstruction of bladder outflow. • There will be urinary stasis: - infection. - stone formation. - tumor. • Readily seen on all imaging , may deform the adjacent bladder or ureter.
Bladder Calcification • Most are bladder calculi. • Usually large and laminated. • Rarely calcification seen in the wall : -Schistosomiasis -Bladder tuumour
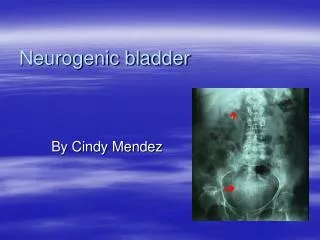
Neurogenic bladder 2 type : • The atonic type: large, smooth-walled baladder , poor or absent contraction and large residual volume. • The Hypertrophic type : regarded as neurologically induced bladder outflow obstruction. small volume, very thick , grossly trabeculated wall and marked sacculation , ureter and PCS may be dilated • Full assessment is by videourodynamics.
Intraperitoneal rupture: - direct blow to the distended UB . - contrast will leak out into peritoneal cavity. • Extraperitoneal rupture: - as part of an extensive injury of fracture of pelvis. - usually in the bladder base. - contrast and hematoma accumulated outside peritoneal cavity and may elevate and compress bladder base
US may show perivesical fluid collection . • Cystography remains the best way of demonstrating actual site of leakage. • If urethral injury suspected , ascending urethrogram should be done before passing any catheter. • CT : demonstrate fresh hematomas or urine collection , and associated fracture.
Prostatic enlargement • Very common in elderly man • Usually benign hypertrophy but may be CA. • Prostatic US: -Transrectal Ultrasound ( TRUS) : can measure the volume and detect relatively small mass. - masses in peripheral zone are usually malignant and in central zone are benign
Transrectal ultrasound guided biopsy is used for diagnoses of prostatic CA. • CT can't demonstrate internal structure , its used for assessing local spread and LNs
MRI : in assessment of early stage of prostatic cancer. • Tumor appear as low signal in the peripheral zone which is high signal on T2 . • It shows extracapsular spread , seminal vesicle invasion and LN metastases
Prostatic calcificaiton • Numerous prostatic claculi. • Very common , that it can be regarded as a normal finding in older men. • No relation to symptoms of BPH or prostatic carcinoma.
Bladder outflow obstruction • Commonest cause of BPH • Other cause : - tumors - Urethral strictures - posterior urethral valve (male infants) - neurogenic obstruction.
US in bladder outflow obstruction • Increased trabeculation and thickness of the bladder wall , with diverticula formation. • PVRU ( residual urine). • Dilatation of collecting system.
Urethral stricture • Usually due to previous trauma or infection • Imaging is by urethrography . • Traumatic stricture : - usually in proximal penile urethra - smooth in outline, relatively short. • Inflammatory stricture ( gonococcal) : - may be seen in any portion of urthera. - usually in anterior urethra
Posterior urethral valve • Commonest cause of BOO in male children . • May be seen antenatally(bilateral hydronephrosis) • US show bilateral hydronephrosis and hydroureter with thick wall bladder. • Can not be diagnoses by retrograde rethrography. • Easily seen on micturatingcystourethrography, as dilatation of posterior urethra terminates abruptly in a convex border formed by the valve
Usually imaging by US , some times MRI. • Scrotal US is done for : > scrotal swelling : - intratesticular ( tumor ) - extratesticular varicocele hydrocele infection (epididymitis,epididmoorchitis) benign epididymal cyst ( common)
Acute testicualr pain and/or swelling: - testicular torsion : dramatic reduction in perfusion on Doppler - acute epididymitis/orchitis: normal or increased perfusion
Ectopic testis ( undescended testis) : - commonest site is in the inguinal canal - MRI used if US inconclusive or ectopic testis lies within the abdomen. MRI produce highly detailed images of scrotal contents and is used in problem solving cases.