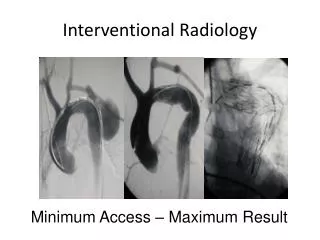
Pediatric interventional catheterization
Learn about balloon septostomy, valvuloplasty, aortic stenosis treatment, and more in pediatric interventional cardiac catheterization. Understand indications, methods, complications, and historical perspectives. Explore outcomes and advancements. Stay informed with Dr. David Shim, MD, from The Heart Center at Children’s Hospital Medical Center in Cincinnati, Ohio.

Pediatric interventional catheterization
E N D
Presentation Transcript
Pediatric cardiac catheterizationPart 1 - balloon proceduresDavid Shim, MDThe Heart CenterChildren’s Hospital Medical CenterCincinnati, Ohio
Pediatric interventional catheterization Diagnosis redirected from catheterization suite to the echocardiography suite Therapy redirected from the surgical suite to the catheterization suite Neonatal caths (Shim et al, 1999) • 1984-5 - 18% interventional (BAS) • 1994-5 - 38% varied interventions (p=0.003)
Balloon septostomy Miller and Rashkind, 1966 Allows mixing in transposition of the great arteries Inflated balloon pulled from left atrium to right atrium Modified use with blade septostomy or static balloon dilation
Balloon valvuloplasty Originally a balloon pull-through Static dilation to separate commissures Success dependant on annulus size and valve morphology Side effect: valve insufficiency
Pulmonary stenosis Kan, 1982 - 1st static balloon dilation Treatment of choice in all centers (>80% success rate) Risk of restenosis 15-20% if dilation required prior to a year of age, rare if over a year old
Pulmonary valvuloplasty Indications • asymptomatic patients with gradients >50 mmHg (Mendelsohn et al - utility of balloon valvuloplasty at gradients >40 mmHg) • symptomatic patients • CHF or cyanosis in the newborn syncope, dyspnea Methods • balloon size equal to 1.2-1.3 times the annulus size
Aortic stenosis Lababidi, 1984 Treatment of choice of many centers Palliative only Methods • single balloon - equal aortic valve annulus (in general, neonates usually require 7 mm balloon) • double balloon - 1.2 times the aortic valve annulus Complication aortic insufficiency
Aortic valvuloplasty Results • Sholler et al, 1988 • demonstrated that balloon:annulus ratio > 1.0 did not improve gradient relief but did increase regurgitation • Rocchini et al, 1990 • 61% acutegradient reduction in 204 patients
Aortic valvuloplasty Results (continued) • Shim et al, 1997 • repeat balloon valvuloplasty resulted in adequate gradient relief in 11/15 patients (73%) while producing worsening aortic regurgitation in 4 patients (27%) - no severe regurgitation - compares favorably to first dilations - 3/4 patients with unsatisfactory gradient relief were on their third aortic valve intervention
Balloon angioplasty Stretch stenotic vessels by creating a tear in the intima and media Risks: rupture or dissection of the vessel (balloon size and inflation pressure) Ideally will grow with patient after relief of obstruction Contraindication: calcification
Balloon angioplasty Pulmonary artery stenosis Coarctation of the aorta Venous (SVC) stenosis Others: baffles, conduits Does not work with pulmonary vein stenosis
Coarctation of the aorta Historical perspective • Sos et al, 1979 and Lock et al, 1982: performed balloon dilation on surgically removed CoA segments • Singer et al, 1982: performed balloon dilation on restenosis of CoA repair • Lababidi et al, 1983: described first balloon dilation on native CoA
Aorta angioplasty Indications • recurrent CoA • - resting gradient >20mmHg, hypertension, and/or symptoms (claudication) • native CoA • - greater than 1 yr old with above
Aorta angioplasty Results (native) • Tynan et al, 1990: VACA study of 140 patients with 82% relief (48+19 to 12+11 mmHg) • Mendelsohn et al, 1994: 78% immediate success rate and 64% positive long-term results • Rao et al, 1996: 77 patients with gradient relief from 46+17 to 11+9 mmHg with restenosis in 83% of neonates, 39% of infants, and 8% of children
Peripheral pulmonary stenosis Historical perspective • Lock et al, 1983 - described balloon dilation of branch pulmonary artery stenosis in 5/7 patients • Rocchini et al, 1984 - described successful dilation in 5 and unsuccessful in 8 patients
Peripheral pulmonary angioplasty Causes • Congenital - TOF, low pulmonary flow - LPA coarctation - Williams, Alagille, and rubella • Acquired - pulmonary emboli • Postsurgical - shunts (Waterston, BT) - Glenn/Fontan anastomosis
Peripheral pulmonary angioplasty Indications • Symptoms of cyanosis, heart failure, or dyspnea • RV pressure of >2/3 systemic • Severe pulmonary insufficiency with MPA pressure >40 mmHg • RV pressure >50 mmHg with unilateral obstruction causing marked disparity in pulmonary blood flow
Peripheral pulmonary angioplasty Results • Kan et al, 1990 - VACA with 182 procedures in 156 patients with moderate results (systolic gradient 49 to 37 mmHg) • Hosking et al, 1992 - VACA follow-up with 53% success in 72 patients • Gentles et al, 1993 - use of high-pressure balloon (17-20 atm) with success rate 63% in previously dilated arteries and 81% in native stenosis