Enhancing Chronic Illness Care: Strategies for Planned Visits and Team Interventions
The presentation from the IDCOP National Summit discusses strategies for improving chronic illness care through organized delivery systems. Key elements include defining team roles, utilizing planned visits for evidence-based care, and fostering effective case management. It emphasizes the value of structured group visits that cater to specific health needs, allowing patients access to varied resources such as specialty services and self-management training. By proactively managing patient care through consistent follow-ups, healthcare teams can ensure better health outcomes and patient engagement.

Enhancing Chronic Illness Care: Strategies for Planned Visits and Team Interventions
E N D
Presentation Transcript
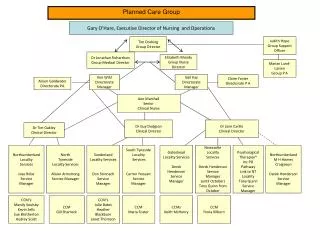
System Changes and Interventions:Planned Care Mike Hindmarsh Improving Chronic Illness Care, a national program of the Robert Wood Johnson Foundation IDCOP National Summit Chicago May 13-15, 2002
Delivery System Design • Define roles and delegate tasks amongst team members. • Use planned visits to support evidence-based care. • Build effective case management skills into practice • Assure continuity by the primary care team. • Assure regular follow-up.
Group Visits: A Primer • Patients brought in by clinically relevant groups • Patients can receive: • Specialty service as needed/available • One-on-one with medical provider • Medication counseling • Self-management support training • Social support • Multiple Models for Group Visits
What is a Planned Visit? • A Planned Visit is an encounter with the patient initiated by the practice to focus on aspects of care that typically are not delivered during an acute care visit. • The provider’s objective is to deliver evidence-based clinical management and patient self-management support at regularly scheduled intervals without the “noise” inherent in the acute care visit.
What does a Planned Visit look like? • The provider team proactively calls in patients for a longer visit (20-40 minutes) to systematically review care priorities. • Visits occur at regular intervals as determined by provider and patient. • Team members have clear roles and tasks. • Delivery of clinical management and patient self-management support are the key aspects of care.
How do you do a Planned Visit? You Plan It!
Step One: Example Senior Care Polypharmacy • Choose a patient sub-population, e.g., all patients >75 on five or more medications • Have programming support person or pharmacy generate list of patients and medications • MD reviews list for patients at highest risk (see handouts)
Step Two: Patient Outreach • RN/LPN/MA checks to see if patient is on any registries • Have PCR call patient and explain the need for planned visit • Allow patient to choose day and time for visit • Ask patient to bring in bag of all medications they are taking (including OTCs and herbals)
Step Three: Preparing for the Visit • RN/LPN/MA prints any relevant patient summaries from registries and attaches to front of chart • MD reviews medications prior to visit, and consults with pharmacy as needed
Step Four: The Visit • Review patient’s medication regimen • Identify and eliminate unnecessary drugs • Adjust remaining medications as needed • Problem solve adherence issues with patient • Create an patient action plan • Schedule follow-up
Follow-up • Does not need to be in-person visit (use phone, email) • Check adherence to action plan • Problem solve as needed • Schedule additional follow-up as needed