Chief Complain & Presentation:
Lemierre’s Syndrome Presenting as a Case of Perforated Otitis Media Vadim Fradlis, DO 1 ; Maya Haasz, MD 2 Department of Emergency Medicine 1 Department of Pediatrics 2 St. Barnabas Hospital, Bronx, NY. Chief Complain & Presentation:. Radiological Findings:. Heme:

Chief Complain & Presentation:
E N D
Presentation Transcript
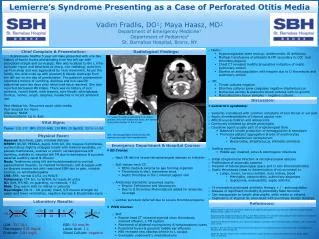
Lemierre’s Syndrome Presenting as a Case of Perforated Otitis MediaVadim Fradlis, DO1; Maya Haasz, MD2Department of Emergency Medicine1Department of Pediatrics2St. Barnabas Hospital, Bronx, NY Chief Complain & Presentation: Radiological Findings: • Heme: • Hypercoagulable state workup: Antithrombin III deficiency • Multiple transfusions of platelets & FFP secondary to DIC and thrombocytopenia • Chest CT revealed multifocal opacities indicative of septic pulmonary emboli • Started on anticoagulation with heparin due to IJ thrombosis and pulmonary emboli • ID: • Throat cultures negative • Otorrhea cultures grew coagulase negative staphylococcus • Numerous aerobic & anaerobic blood cultures with no growth • Mastoidectomy tissue samples – negative cultures A previously healthy 5 year old male presented with one day history of tactile fevers and bleeding from the left ear with associated otalgia and cervicalgia. Pain was localized to the L infra-auricular region and described as sharp, non-radiating, woke him up from sleep and was aggravated by neck movement. As per the family, the child woke up with purulent & bloody discharge from the left ear on the day of presentation. The patient’s grandmother reported a history of vomiting, diarrhea and non-specific abdominal pain two days prior which had since resolved. She also reported decreased PO intake. There was no history of sick contacts, recent travel, neck trauma, sore throat, odynophagia, tinnitus, rashes, cough, dyspnea, headaches or recent antibiotic use. Past Medical Hx: Recurrent acute otitis media Past Surgical Hx: None Allergies: NKDA Immunizations: Up to date General: Non-toxic, calm, minimal distress HEENT: NC/AT, PERRLA, pupils 3mm b/l, dry mucous membranes, erythematous slightly enlarged tonsils with minimal exudates, no pseudo-membranes, vesicles or ulcers; serosanguenous left otorrhea, inability to visualize left TM due to edematous & purulent external auditory canal & effusion Neck: Tenderness along left sternocleidomastoid to cervical paravertebral muscles, no mastoid tenderness; soft & supple with no discreet masses but with restricted ROM due to pain, notable trismus, no lymphadenopathy CVS: RRR, normal S1/S2, no M/G/R Pulmonary: CTA b/l, no W/R/R, b/l equal air entry GI: Soft, NT/ND, no guarding, no rebound, + BS Skin: Dry, warm with no rashes or petechia Neurologic: CN II – XII grossly intact, 5/5 muscle strength b/l upper and lower extremities, negative Kernigs & Brudzinskis signs. R L R L Discussion: • Lemierre’s syndrome: • Seldomly considered with common complains of sore throat or ear pain • Septic thrombophlebitis of internal jugular vein • Affects young children and adolescents • Commonly heralded by simple pharyngitis • Causative agent usually part of oropharyngeal flora • Bacteria’s innate production of hemagglutinin & hemolysin • Promotes platelet aggregation & lysis of erythrocytes • Fusobacterium necrophorum • Bacteroides, Streptococcus, Eikinella corrodens • Inciting sources: • Middle ear, mastoid, sinus & odontogenic infections • Initial streptococcal infection retropharyngeal abscess • Proliferation of anaerobic bacteria • Invasion of lateral pharyngeal space and IJ vein thrombophlebitis • Septic thrombosis leads to dissemination of micro-emboli to: • Lungs, bones, nervous system, liver, kidney, blood • Meningitis, osteomyelitis, pulmonary abscesses • Septicemia, endocarditis, septic arthritis • Tx necessities prolonged antibiotic therapy + / - anticoagulation • Disease of significant morbidity & potentially fatal outcome • Can masquerade as simple pharyngitis, otitis media or externa • Cognizance of atypical Sx associated with seemingly benign illnesses CT: septic thrombus extending from distal portion of the left transverse sinus, the siphon, & proximal portion of the IJ vein MRI: thrombophlebitis involving the left sigmoid sinus and left otomastoiditis Vital Signs: Temp: 102.2ºFBP: 93/55 HR:139 RR: 20SpO2: 100% on RA Physical Exam: Emergency Department & Hospital Course: • ED Course: • Neck XR did not reveal retropharyngeal abscess or infection • Soft tissues neck CT: • Otitis media & externa by gas forming organism • Thrombosis in the L transverse sinus • Septic thrombus in the L internal jugular vein • Antibiotics started for presumed sepsis: • Empiric Ceftriaxone and Vancomycin • Due to IJ thrombus Metronidazole added for anaerobic coverage • Lumbar puncture deferred due to severe thrombocytopenia • PICU Course: • ENT: • Repeat head CT revealed sigmoid sinus thrombosis, mastoid effusion, L TM rupture • Placement of bilateral myringotomy & tympanostomy tubes • Persistent fevers & purulent middle ear effusions • MRI revealed new abscess inferior to L occiput • Eventually underwent L mastoidectomy Laboratory Results: References: Bondy P, Grant T. Lemierre’s syndrome: What are the roles for anticoagulation and long-term antibiotic therapy? Ann Otol Rhinol Laryngol. 2008;117:679–83. Goldenberg, NA, Knapp-Clevenger, R, Hays, T, and Manco-Johnson, MJ. Lemierre’s and Lemierre’s-Like Syndromes in Children: Survival and Thromboembolic Outcomes. Pediatrics 2005;116:e543–e548. Ridgway JM, Parikh DA, Wright R, et al. Lemierre syndrome: a pediatric case series and review of literature. Am J Otolaryngol 2010; 31:38. Ruirdan T. Human infection with Fusobacterium necrophorum (Necrobacillosis) with a focus of Lemierre’s syndrome. Clin Microbiol Rev. 2007;20:622–59 Weeks DF, Katz DS, Saxon P, et al. Lemierre syndrome: report of five new cases and literature review. Emerg Radiol 2010;17:323Y328. 130 98 8 10.0 13 107 12.8 27.0 19.6 28.3 3.1 24 0.5 1.2 LDH: 337 IU/L ESR: 60 mm/Hr Fibrinogen: 578 mg/dl Lactic Acid: 1.1 D-dimer: 3.81 mg/L Blood Culture: negative