TRACTION
TRACTION. OUTCOMES. Must be familiar with the types of mechanical traction. Must be familiar with the mechanical effects of traction. Must be familiar with the indications for mechanical traction . Must be familiar with the contra-indications for mechanical traction.


TRACTION
E N D
Presentation Transcript
OUTCOMES Must be familiar with the types of mechanical traction. Must be familiar with the mechanical effects of traction. Must be familiar with the indications for mechanical traction. Must be familiar with the contra-indications formechanical traction.
OUTCOMES Must be familiar with the application and technique for mechanical cervical traction. Must be familiar with the dosage and progression of mechanical cervical traction. Must be familiar with the application and technique for mechanical lumbar traction. Must be familiar with the application and technique for mechanical lumbar traction.
DEFINITION Traction is derived from the Latin word “tractico” which means a process of drawing or pulling. It is used in the same way as ordinary passive mobilisation techniques
TYPES OF TRACTION • Continuous traction • Sustained traction • Intermittent traction • Manual traction • Auto-traction • Positional traction • 90/90 traction
TYPES OF LUMBAR TRACTION • Inversion traction • Gravity traction • Pool traction
MECHANICAL EFFECTS • Delordosis of the spine • Separation of the vertebrae • Widening of intervertebral foramen • Combination of distraction and gliding of the facet joints • Stretching of spinal musculature and ligaments • Distraction
MECHANICAL EFFECTS • Tensing of posterior longitudinal ligament • Suction • Relaxation of spinal muscles • Joint mobilisation • Reduction of herniated nuclear material • Increase of interspinous distances • Epidural fatty tissue become prominent
MECHANICAL EFFECTS • Small pressure changes • Normalisation of conduction • Pain relief
Onel (1989) - negative intradiscal pressure “sucks back” the herniated nucleus material and widening of IV disc space causes a stretch on the ant and post longitudinal ligaments MECHANICAL EFFECT (SUCTION)
Krause (2000) negates this statement MECHANICAL EFFECT (SUCTION)
CLINICAL EFFECTS OF TRACTION • Remains controversial • Produced from combination of mechanical and physiological effects
Severe nerve root pain Recent neurological changes Degenerative conditions Widely distributed areas of thoracic and lumbar pain Pathological Trauma to ligaments Spondilolisthesis and spondilolysis No further improvement with mobilisation Lumbar conditions where movements are painless during objective evaluation INDICATIONS
Resent onset of severe lumbar pain Hypermobility or instability Undiagnosed pain Persistent cough Cardio-vascular conditions Spinal malignancy Cord compression Spinal infection Hiatal hernia Uncontrolled hypertension Aortic aneurysm Abdominal hernia Severe haemorrhoids CONTRA-INDICATIONS
CONTRA-INDICATIONS • Inadequate investigation • Acute traumatic lesions • Large central disc • Ileofemoral incompetency • Uncooperative patient • Marked ligamentous insufficiency and segmental instability
CONTRA-INDICATIONS • Dizzy, nauseated and sick after first careful attempt - cervical • Vertebrobasilar insufficiency • Patient unable to relax - cervical • Appreciable involuntary head or neck movements - cervical
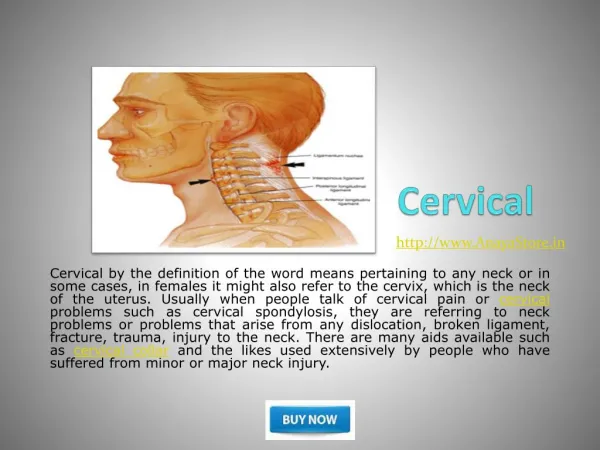
Upper cervical area C1-C4 Neutral position UPPER CERVICAL TRACTION
Lower cervical area C4-T1 Neck in flexion using pillows or towel roll LOWER CERVICAL TRACTION
METHOD • Patient lies with two pillows under his knees • Apply gentle traction via spreader bar • Know the area and severity of patient’s pain • Trial-run for 10 seconds • Re-assess the symptoms
PROGRESSION • Applied daily • Test neck movements directly after traction except with severe nerve root pain • Time should be increased first • Strength can be increased in small stages • Treatment usually 15 minutes • Severe nerve root: 30 minutes
PROGRESSION • Stop traction if no improvement after 4-5 treatments • Severe nerve root pain sometimes at least 7-8 treatments, but • Movement test must improve by 4th to 5th session • NB: Carefully assess signs and symptoms before, during and after treatment
UPPER LUMBAR TRACTION • L1-L4 • Neutral position
L4-S1 Patient positioned in Fowler’s position (Thomas-curl position) LOWER LUMBAR TRACTION
LUMBAR TRACTION • Attach the thoracic harness in standing and re-adjust in supine • Assess area and degree of pain before pull • Knees flexed over pillows to put joint in mid-position • Trial run
12,5 kg to 13 kg for 10 seconds Arms by side Reduce if patient experiences low back pain Re-assess back and leg symptoms after 10-20 seconds LUMBAR TRACTION
DURING RELEASE • Rolling pelvis side to side • Rest for a few minutes • NB: Do not test patients comparable sign immediately only re-assess following day • Warn patient
PROGRESSION • Pain less or gone = improvement • Signs and symptoms worse • Signs and symptoms ISQ • Over 3-4 sessions improvement will be small • If signs improve - increase time first • With no exacerbation - increase kg
REMEMBER • There is often a postural component involved with disorders of the lumbar spine
RULE OF PROCEDURE (Grieve, 1989) • Bear in mind contra-indications • Examine thoroughly • Try and localise the problem • Keep treatment under control by frequent reassessment and precise recording • Each step should be reasoned • Modify techniques which are unproductive
RULE OF PROCEDURE (Grieve, 1989) • Warn patient about treatment soreness • Do not over treat • Never push through spasm • Treat joint irritability with respect
TREATMENT PROTOCOL • Teach spinal stabilisation • Dynamic maintenance of postural control • Patient reassurance • Ergonomic advice • Mechanical principles involved • Restoration of maximal patient function • Pain control
TREATMENT PROTOCOL • To educate patient • To maintain lumbar muscles • Combination of treatments • Back school • Strengthening exercises
TREATMENT PROTOCOL • Flexibility exercises • Fitness • Total bedrest • Encouragement to function despite symptoms • Corset • Lumbar intervertebral traction