Download
1 / 28
290 likes | 484 Vues
And then what?. Patient Care Doesn ’ t End at Discharge. “ Can I get a Med Rec? ”. Heath Denmark, PA-SII South University c/o 2013 May 10, 2012. Alper E, O ’ Malley TA, Greenwald J. Hospital Discharge. UpToDate.com. Dec 19, 2011. Time for Discharge.

E N D
And then what? Patient Care Doesn’t End at Discharge “Can I get a Med Rec?” Heath Denmark, PA-SII South University c/o 2013 May 10, 2012 Alper E, O’Malley TA, Greenwald J. Hospital Discharge. UpToDate.com. Dec 19, 2011
Time for Discharge Discharge planning is a mandatory complex process that seeks to determine the appropriate level of services required by the patient and then match the patient to an appropriate site of care. This process ideally begins at the start of the hospitalization
Discharge Process Elements Discharge planning Medication reconciliation Discharge summary Patient instructions Discharge checklist
Post-Discharge Site of Care • When it has been determined that a patient is medically ready for discharge, the health care team must determine the most appropriate setting for ongoing care. • Need to consider: • Medical • Functional • Social
Home? • Must consider these factors first: • Patient cognitive status • Patient activity level and functional status • The nature of the patient's current home and suitability for the patient's conditions (eg, presence of stairways, cleanliness) • Availability of family or companion support • Ability to obtain medications and services • Availability of transportation from hospital to home and for follow-up visits • Availability of services in the community to assist the patient with ongoing care
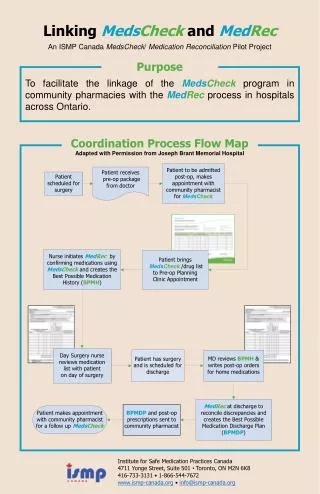
Medication Reconciliation Gillespie U, Alassaad A, Henrohn D, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med 2009; 169:894 • Accurate list of home meds • Needs to be updated • Accurate list of medications being taken at time of discharge • Indications for each medication changes or initiation of new meds • In Sweden, patients 80 years or older who were randomly assigned to receive a medication reconciliation intervention by unit-based pharmacists had 16 percent fewer visits to the hospital and 47 percent fewer emergency department visits than controls. Medication-related readmissions were reduced by 80 percent.
Unresolved Issues with Med Recs Who should perform medication reconciliation (eg, nurse, pharmacist, physician)? How can resources (personnel, systems) be most effectively allocated to perform medication reconciliation, and reimbursement attached to safety-oriented, time-consuming tasks such as medication reconciliation? How should one determine the "gold standard" list of medications for individual patients, to use as the basis for reconciliation? How can aftercare providers reliably be informed of medication changes in a timely and accurate fashion? How can patients and family/caregivers be engaged in understanding the importance of medication reconciliation?
Important Elements ofDischarge Summary The outcome of the hospitalization The disposition of the patient Provisions for follow-up care including appointments, statements of how care needs will be met, and plans for additional services (eg, hospice, home health assistance, skilled nursing)
Patient Instructions • One model for patient materials, developed by the National Patient Safety Foundation, is called Ask Me 3. • What is my main problem? • What do I need to do? • Why is it important for me to do this? • Discharge instructions, both written and verbal, should be reviewed with the patient/family caregivers with an emphasis on assessing and ensuring comprehension.
Factors Contributing toRehospitalization van Walraven C, Bennett C, Jennings A, et al. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ 2011; 183:E391. • Many rehospitalizations are unavoidable • Progression of disease process • Separate problem unrelated to initial admission • Patient not following through with initial discharge plan • However, many are also preventable • Systemic review of 34 studies found that the median proportion of readmissions deemed avoidable was 27% but what was deemed “preventable” was varied between the studies.
Modifiable Factors of Rehospitalization • Several factors that increase the likelihood of rehospitalization may be modifiable • Premature discharge or inadequate post-discharge support • Insufficient follow-up • Therapeutic errors • Adverse drug events and other medication related issues • Failed handoffs • Complications following procedures • Nosocomial infections, pressure ulcers, and patient falls.
Therapeutic Error • Medication error occurs in approximately 20% of patients post-discharge • Examples of these types of errors include: • Patients sent home without prescriptions for necessary medications • Patients receiving duplicate prescriptions for medications they have at home labeled with different name (eg, generic and proprietary names) • Inadequate monitoring and follow-up for drug side effects
Failed Handoffs • Poor information transfer from hospital-based providers to primary care providers occurs commonly • Tests that are pending at discharge often fail to be communicated to providers responsible for their follow-up
Failed Handoff cont. Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med 2005; 143:121 Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA 2007; 297:831. In one study, 41 percent of discharged patients had a test pending at discharge. Almost one in ten patients potentially required an intervention, but almost two-thirds of responsible aftercare providers were unaware that a test was outstanding. A meta-analysis revealed that only 12 to 34 percent of discharge summaries had reached aftercare providers by the time of the first post hospitalization appointment
Absent or Delayed Follow Up Most studies affirm that patients who are scheduled or seen for post hospital follow-up are less likely to be readmitted
High Risk Patients Screening for increased risk may help healthcare providers and organizations target resources to patients most likely to be rehospitalized.
Clinical factors to consider for risk assessment • Use of high risk medication • antibiotics, glucocorticoids, anticoagulants, narcotics, antiepileptic medications, antipsychotics, antidepressants, and hypoglycemic agents • Polypharmacy (five or more medications) • Specific clinical conditions • eg, advanced COPD, diabetes, heart failure, stroke, cancer, weight loss, and depression
Demographic factors to consider for risk assessment • Prior hospitalization, typically including unplanned hospitalizations within the last 6 to 12 months • Black race • Low health literacy • Reduced social network • i.e. Living alone with little or no contacts
Post Discharge Interventions Follow-up Phone call Communication with ambulatory provider Home visits
Phone Call Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med 2001; 111:26S. Balaban RB, Weissman JS, Samuel PA, Woolhandler S. Redefining and redesigning hospital discharge to enhance patient care: a randomized controlled study. J Gen Intern Med 2008; 23:1228 Calls have been moderately effective at reducing emergency department visits and improving follow-up with providers, but demonstrated a trend towards reduced hospital readmissions in only one study
Home Visits Stewart S, Pearson S, Horowitz JD. Effects of a home-based intervention among patients with congestive heart failure discharged from acute hospital care. Arch Intern Med 1998; 158:1067. One trial illustrated that a single home visit by a nurse and pharmacist to patients discharged with a diagnosis of heart failure, with a goal of optimizing medication management, showed a trend towards almost a 50 percent reduced risk of unplanned readmission
Telemonitoring • Using an integrated telephonic stethoscope in conjunction with follow-up nursing calls in patients with heart failure reduced emergency department visits in one small study, and demonstrated a trend toward reduced readmissions and overall costs. • blood pressure • heart rate • weight • Oxygen saturation
Multidisciplinary Team Effort A nurse discharge advocate to assist with discharge planning and preparation A clinical pharmacist to call the patient 2-4 days following hospital discharge, to review the medication list, address any medication questions or concerns, reinforce the plan, and assess for adverse effects related to medications Follow-up appointments scheduled at times convenient to the patient Medication reconciliation A low literacy discharge instruction booklet for patients, also provided to the primary care clinician
H2H A new quality improvement initiative by the American College of Cardiology (ACC) and the Institute for Healthcare Improvement (IHI) called Hospital to Home (H2H) was developed to help in this endeavor. The program was designed to improve patient outcomes and decrease readmission rates for cardiovascular patients, specifically heart failure (HF) and acute myocardial infarction (AMI) patients. The goal of the H2H initiative is to decrease HF and AMI readmission rates by 20% by the year 2012
Summary Several systems initiatives have shown promise in minimizing rehospitalizations. These interventions include improved collaboration between the care team, patient, and aftercare provider prior to discharge; medication reconciliation; enhanced patient education and empowerment; home visits or telephone calls by clinical providers; remote monitoring; and early post-discharge follow up. Patient instructions should take into account the patient's cognitive status, health literacy, and other barriers to self-care. Multiple concurrent interventions may be more effective than single components.