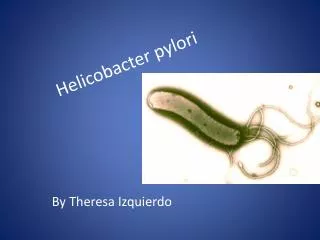
Helicobacter pylori
Helicobacter pylori. Brianán McGovern (microbiology spR). Background. 1983-discovered by Warren and Marshall in Australia Discovery revolutionised the treatment of duodenal and gastric ulcers Earned them the Nobel Prize for Medicine in 2005 Formerly known as Campylobacter pyloridis.

Helicobacter pylori
E N D
Presentation Transcript
Helicobacter pylori Brianán McGovern (microbiology spR)
Background • 1983-discovered by Warren and Marshall in Australia • Discovery revolutionised the treatment of duodenal and gastric ulcers • Earned them the Nobel Prize for Medicine in 2005 • Formerly known as Campylobacter pyloridis
Nearly 20 species of Helicobacter are now recognised • The gastric helicobacters colonise the stomachs of animals. The monkey, cat, dog, cheetah all harbour their own species • H. cinaediand H. fennelliaeare associated with proctitis in homosexual men • H. pylori are found in the human stomach. Molecular studies suggest transmission from an animal source.
Helicobacter pylori McColl K. N Engl J Med 2010;362:1597-1604
Description • Gram-negative spiral bacillus • Fastidious in terms of growth requirements • :strictly micro-aerophilic • :require C02 for growth • :on charcoal medium • Has a tuft of sheathed unipolar flagella; specially adapted to colonise mucous membranes
Gram stain of H. pylori recovered from an individual without prior antimicrobial therapy. Organisms display typical ‘seagull’-like appearance.
Hallmark of the species is production of urease enzyme • -urease breaks urea down to C02+NH3 • -amonia is a strong base • -process helps H. pylori survive • strongly acidic stomach conditions • Very fragile (a point of importance • when referring samples to the lab)
Epidemiology • H. pylori infection occurs worldwide • Prevalence varies greatly among countries and population groups • 20 – 50% prevalence in middle age adults in industrialised countries • >80% prevalence in middle age adults in developing countries • :may reflect poorer living conditions
Transmission • Oral ingestion of bacterium • within families (esp children) • person-person contact • faecal-oral transmission • ?role of waterborne transmission • Usually contracted in the first 2 years of life
Site of infection • Highly adapted organism that lives only on gastric mucosa • Gastric antrum is the most favoured site • Present in the mucus that overlies the mucosa
Gastric-biopsy specimen showing Helicobacter pylori adhering to gastric epithelium and underlying inflammation McColl K. N Engl J Med 2010;362:1597-1604
Course of infection • After several days incubation period, patients suffer mild attack of acute gastritis • -abdominal pain • -nausea • -flatulence • -bad breath • Symptoms last about 2/52 but hypochlorhydria can last up to one year
Despite a substantial ab response, infxn and chronic gastritis persist • After decades there may be progression to atrophic gastritis (conditions which are inhospitable for the bacteria) and numbers reduce
The outcome of infection by H. pylori reflects an interaction between:
H. pylori infection directly associated with • PUD • -lifetime risk 3% in US, 25% Japan • -eradication provides long-term cure • Gastric carcinoma • -strong evidence of increased risk 0.1-3% • -unclear whether eradication reduces the risk of gastric cancer • MALT lymphoma • -72%→ 98% of MALT lymphoma infected with H. pylori
H. pylori may be implicated in:- • Non-ulcer dyspepsia • -increased prevalence of H. pylori but data inconsistent (symptomatic improvement only 9%) • -little evidence that chronic H. pylori infection in the absence of ulceration causes upper GI symptoms • GORD • -recent meta-analysis : no significant association
Laboratory diagnosis:non-invasive tests • Serology : detect an immune response by examining a blood sample for abs to the organism (ELISA) • : poor accuracy • Urea breath test : a urea solution labelled with C14 isotope is given to pt. The C02 subsequently exhaled by the pt contains the C14 isotope and this is measured. A high reading indicates presence of H. pylori
Faecal antigen test : detect H. pylori antigens in faecal specimens • Polymerase chain reaction (PCR) : can detect HP within a few hours. Not routine in clinical use.
Invasive testing • Histological examination of biopsy specimens of gastric/duodenal mucosa take at endoscopy • CLO-test ® : based again on urease-production by the organism->NH3 production->rise in pH=>change in the colour indicator of the kit • -High sensitivity and specificity • -Prompt result
Invasive testing • Culture : • -no more sensitive than skilled microscopy of histological sections • -used for antibiotic resistance testing • -requires selective agars and incubation periods
Tests for Helicobacter pylori Infection McColl K. N Engl J Med 2010;362:1597-1604
Indications for therapy • Strongly recommended • Duodenal or gastric ulcer • MALT lymphoma • Atrophic gastritis • Recent resection of gastric cancer Maastricht 2-2000 Consensus Report
Indications for therapy • Treatment advised • Functional dyspepsia • Gastro-oesophageal reflux disease (patients requiring long-term acid suppressive therapy) • Use of NSAIDs Maastricht 2-2000 Consensus Report
Treatment • Goal of treatment to eradicate infection • Triple therapy regimens consist of one anti-secretory agent and two antimicrobial agents for 7 to 14 days • Triple therapy regimens must • have cure rate of approximately 80% • be without major side effects - minimal induction of resistance
First line treatment • Combination of two or more antimicrobial agents increases rates of cure and reduces the risk of selecting for resistant H. pylori • Many factors may result in failure of treatment • microbial factors • patient compliance • geographical differences
First line therapy • PPI b.d. + clarithromycin 500mg b.d. • + • amoxicillin 1000mg b.d. or metronidazole 400mg BD minimum of 7 days • In case of failure • Second line therapy • PPI b.d. + bismuth subsalicylate/subcitrate 120mg QDS + metronidazole 500mg t.d.s. + tetracycline 500mg q.d.s. • for a minimum of 7 days • If bismuth is not available, PPI based triple therapies should be used • Subsequent failures should be handled on a case-case basis. Patients failing second-line therapy in primary care should be referred Maastricht 2-2000 Consensus Report
Guidelines for Evaluation and Management of Helicobacter pylori Infection McColl K. N Engl J Med 2010;362:1597-1604
Reinfection • Reinfection following successful bacterial cure is unusual • Commonly represents recrudescence of the original bacterial strain • In adults, reacquisition of the bacteria occurs in <2%/persons/year which is similar to the rate of primary infection in adults
Failure of treatment • Failure of initial course occurs in 1 in 5 • 2nd-line Tx : • either an alternative regimen • quadruple Tx (PPI+bismuth+2 antibx)
Key points • -> H. pylori is a flagellated spiral micro-aerobe • -> Infection is a risk factor for gastric cancer • -> Causes PUD and gastritis • -> Produces a cell-damaging toxin • -> Transmission route is unclear • -> Dz rates are falling in industrialised countries • -> Tx is by eradication using combination therapy
Recommendations • The noninvasive test-and-treat strategy for H. pylori infection is reasonable for younger patients who have upper gastrointestinal symptoms but not alarm symptoms • Noninvasive testing can be performed with the use of the urea breath test, fecal antigen test, or serologic test; the serologic test is the least accurate • Triple therapy with a proton-pump inhibitor, clarithromycin, and amoxicillin or metronidazole remains an appropriate first-line therapy • Recurrence or persistence of symptoms after eradication therapy for uninvestigated dyspepsia is much less likely to indicate that treatment has failed than to indicate that the symptoms are unrelated to H. pylori infection.
Recommendations • Further eradication therapy should not be considered unless persistent H. pylori infection is confirmed • Data are lacking to inform the optimal management of recurrent or persistent dyspepsia after noninvasive testing and treatment of H. pylori infection • Options include symptomatic acid-inhibitory therapy, endoscopy to check for underlying ulcer or another cause of symptoms, and repeat of the H. pylori test-and-treat strategy; other potential reasons for the symptoms should also be reconsidered
Clinical PracticeHelicobacter pylori Infection Kenneth E.L. McColl, M.D. N Engl J Med Volume 362(17):1597-1604 April 29, 2010 Thanks for your attention!