Helicobacter pylori
Helicobacter pylori. Dr.B.Boyle. History Introduction Microbiology Epidemiology and Transmission Pathogenesis. Clinical Outcomes of Infection Diagnosis Treatment Options Future. Contents/Aims of Lecture. Objectives: to have a clear understanding of disease caused by

Helicobacter pylori
E N D
Presentation Transcript
Helicobacter pylori Dr.B.Boyle
History Introduction Microbiology Epidemiology and Transmission Pathogenesis Clinical Outcomes of Infection Diagnosis Treatment Options Future Contents/Aims of Lecture Objectives: to have a clear understanding of disease caused by Helicobacter pylori in terms of the above headings
Helicobacter pylori History • In 1982 following the Easter holidays in the Microbiology Dept of the Royal Perth Hospital a culture of a spiral-shaped bacterium from gastric biopsies of patients with gastritis was isolated • The discovery was by Dr.Robin Warren and Dr.Barry Marshall
Introduction • This discovery have revolutionised the diagnosis, treatment and prognosis of upper gastrointestinal disease • H.pylori causes gastritis in over half of the world`s population and is the aetiological agent of 95% of duodental ulcers, 70-80% of gastric ulcers and has casual rate in probably up to 60-70% of Gastric Cancer
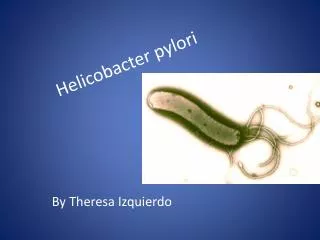
H.pylori -Microbiology • Small curved microaerophilic gram-negative rods 2-4ųm long • Selective medium required for isolation-10% sheep blood agar + selective antibiotic supplement • Incubated at 80-85% N2, 5-10% CO2, 5-10% H2 O @ 37ºC • Identified by urease, oxidase, catalase
Basis of Urease Test NH2 Urease 2NH3+ + CO2 H 2O C O + NH2 Ammonia formed results in ⇈pH
Epidemiology • Infection occurs worldwide • Prevalence will depend on the country and population groups • Overall prevalence strongly correlates with socio-economic conditions • In Middleaged adults in developing countries prevalence is 80%, in industralised countries 20-50% ( rate of acquistion decreasing) • Acquisition:Oral Ingestionof the bacterium • Transmission:Within families in early childhood, not isolated from water etc, e
Epidemiology • H.pylori infection in adults is usually chronic without specific therapy: on the other hand , spontaneous elimination of the bacterium in childhood is probably relatively common • NEJM , Vol. 347, No. 15 Oct 10, 2002 mm.HH
The anatomical regions of the stomach, showing the common location of ulcers (X)
Pathogenesis • H. pylori is found only on gastric epithelium where the organisms tend to cluster around the junctions between cells and virtually never penetrate the cells themselves. • H. pylori is able to survive in the gastric environment which is hostile to growth of most bacteria.
Figure 2. Pathogen–Host Interactions in the Pathogenesis of Helicobacter pylori Infection.
Pathogenesis • Factors permitting colonisation: • (i) Spiral shape and flagellate – for motility within this mucous layer. • (ii) Urease activity – which generate ammonium ions that buffer gastric activity • (iii) Micro-aerophilism – for survival within the mucous gel • (iv) Attachment to epithelial cells • (v) Evasion of Immune response
Pathogenesis Vac A Vac A Gene Variants , More severe disease H.pylori Genome Changes continuously Hop Proteins, Adhesins Cag Pathogenicitiy Island, translocates CagA into host cell ,phosphorylated , Binds SHP-2 TP→ Growthfactor-like Cellular response and Cytokine production by Host cell Bab A adhesin, Binds fucosylated Lewis B Blood group antigen Ure 1, p H Gated urea channel
Pathogenesis • Hop proteins-enzymes which modify the antigenic structure of surface molecules, control entry of foreign DNA into bacteria and influence motility • VacA-95 kd protein, vaculoating cytotoxin inserts itself into the epithelial cell membrane and forms a hexameric anion-selective, voltage dependent channel, in through which nutrients like HCO3- and organic anions can be released and targets mitochondrial membrane inducing apoptosis
Figure 1. The cag Pathogenicity Island. Virtually all patients with Duodenal ulcer have cag-PAI + strains
Figure 2. Pathogen–Host Interactions in the Pathogenesis of Helicobacter pylori Infection.
Host Response to H.pylori • H.pylori causes continuous gastric inflammination in virtually all infected persons • Host response triggered by attachment to gastric epithelium (Class II MHC-apotosis) • Initially neutrophils then T and B cells,plasma cells and macrophages • Role of cag-PAI(Stronger response IL8) and transolation of Cag A into gastric cells, Urease contributes • Infected gasric epithelium have increased levels of interleukin-1ß, interleukin-2,interleukin 6, interleukin-8 and TNFà.Interleukin 8 key role
Host Response to H.pylori • H.pylori induces a strong systemic and mucosal humoral response • This does not eradicate the pathogen but leads to further damage (useful in diagnosis) • For example : HP infected individuals may have an autoantibody response resulting in atrophy of the corpus due to antibodies against H+/K+ -ATPase of gastric pariental cells
Host Response to H.pylori • Although the pathogen is extracellular the T cell response of the gastric mucosa is Th1 , the resulting cytokines from Th1 response (Interleukin 2 and Interferon –ŷ) promote gastritis( whereas Th2 cytokines are protective) • The Th1 response may be due in part to antral production of Interleukin 18 • The Th1 response and Fas mediated apoptosis may favour survival of the organism
Gastrin/Somatostatin (Duodenal Ulcer,H.pylori infected) • Bacterial products e.g Urea • Inflammatory mediators e.g Interleukin 1B, TNF) • Histamine relase from Mast cells Low gastric somatostain level 6x↑Gastrin Releasing Peptide( mediates release of Gastrin, group of Peptide hormones produced by antral G cells), more if Cag A + strain ↑HyperGastrinaemia ↑Pariental cells mass( body) ↠Hypersecretion Acid May be genetic determinant of more response to Gastrin (if D.U ↑ basal secretion of acid secretion)
H+ D cellsomatostatin Parietal cell Antral G cellGastrin Mast cellHistamine (+) (–) (+) (–) (+) (–) The hormonal control of acid secretion
Activated netrophils release oxygens and nitrogens radicals Chronic inflammination leads to epithelial cell turnover and apoptosis ( Fas mediated contact ILY and Th1) Proinflamminatory polymorphisms of the Interleukin -1ß gene favour the development of gastritis in the body of the stomach associated with hypochlorhydria, gastric atrophy and gastriccarcinoma ( Fas, NF-KB AND map kinases) In the absence of POLY, HP mediated gastritis develops predominately in the antrum with normal to high level acid secretion, leading to Duodenalulcer or Asyptomatic infection Other Methods of Epithelial Damage
Clinical Outcome • This is determine by Host and Pathogen factors • H.pylori is responsible for the majority of duodenal and gastric ulcers(50-80% of benign) • The lifetime risk of peptic ulcer is 3% in U.S. and 25% Japan-Treatment for HP lowers recurrence rate • 1994 H.pylori was classified as a type 1- definite carcinogen • Uemura et al 2001 1526, 2.9% of 1246 patients infected with H.pylori developed Gastric Cancer over 7.8 years as compared to none of 280 controls non-infected or 253 treated group
Clinical Outcome • H.pylori Infection increase risk of MALT lymphoma and 72-98% of pts with MALT lymphoma are infected • Therapy causes regression of MALT lymphoma in 70-80% cases • The role of H.pylori Infection in dyspepsia not associated with ulcers
Diagnosis Non-invasive [13C] Urea Breath Test [14C] Urea Breath Test ELISA( Serology) Stool Antigen Test- may be ideal in children , follow up after 8 week interval ( not on table), Invasive Culture Histology Urease Consider Test of Cure
MODALITY ADVANTAGES DISADVANTAGES Endoscopy with Biopsy ( must be performed symtoms of Gastriccarcinoma or > 50Years) Permits inspection of pathology, allows detention of ulcers, neoplasms. Invasive, expensive, time consuming. Culture Performed in those Who have failed 2nd Line therapy Permits determination of antimicrobial susceptibilities and pathogenic features of isolates. Not optimally sensitive in most laboratories. Requires several days for results. Histology Generally more sensitive than culture. Allows direct visualisation of organism and extent and nature of tissue involvement. Gastritis may be patchy and biopsy may be performed on wrong area. Insensitivity to detect small numbers of organisms. Requires several days for results. Diagnosis
Urease Detection Rapid, most positives seen within 2 hours Increased sensitivity requires longer incubation. May be false positives with bacterial overgrowth. Serology Not reliable in young children Noninvasive, rapid, quantitative, inexpensive. No determination of lesions or pathology, no antimicrobial susceptibility. Not rapidly responsive to therapy. Urea Breath Tests 90% sensitivity and specificity Relatively non-invasive, relatively rapid, quantitative, rapidly responsive to therapy. Most valuable for assessing response to eradication therapy after 4-8 weeks. Involves expensive instrumentation or administration of radioisotopes. More invasive and less convenient than serology. No determination of lesions or pathology, no antimicrobial susceptibility. Diagnosis
Stool Antigen Test • Advantages : non-invasive , EIA format, easy to automate , results in hours, improving with Monoclonal design • Disadvantages: Not as good Negative predictive value as UBT, Kits vary
Therapy • The Goal of therapy is eradication of the organism as if this is achieved reinfection rate are low and the benefit of treatment is longterm • 2 antimicrobials reduces the selection of resistance • Testing for Infection only required if treatment is intended • If test for H.pylori positive , use eradication therapy
Standard triple therapy-Eradication therapy, which is probably the most widely used treatment for eradication of H. pylori.-7days mimimal Proton pump inhibitor B.D. (e/g Lansoprazole 30 mg BD) + Clarithromycin 500mg B.D. 1/52 90% plus effective + Amoxycillin 1g B.D. Or If penicillin allergic Proton pump inhibitor B.D. (e/g Lansoprazole 30 mg) Clarithromycin 500mgB.D. Metronidazole 400 mg B.D If treatment failure refer to Gasterenterologist
Resistance to therapy • Geographical variation, depends on surveillance • Approx, 10% to clarithromycin • Approx. 30-50% to metronidazole in some studies • Treatment success correlates with compliance and active therapy
FUTURE • ?Vaccination- possibly therapeutic or preventative • Eluciadation of the Immunology of the human stomach
SUGGESTED READING NEJM , Vol. 347, No. 15 Oct 10, 2002