Cohort studies Case control studies Field methods
Cohort studies Case control studies Field methods. Every epidemiological study should be viewed as a measurement exercise Kenneth J. Rothman, 2002. What does this mean?. Cohort study. What is a cohort study? Types of cohorts: Observational - retro, prospective, Clinical trials Other?

Cohort studies Case control studies Field methods
E N D
Presentation Transcript
Every epidemiological study should be viewed as a measurement exercise Kenneth J. Rothman, 2002 What does this mean?
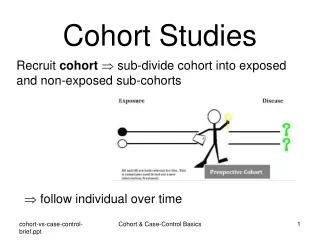
Cohort study • What is a cohort study? • Types of cohorts: • Observational - retro, prospective, • Clinical trials • Other? • What is a fixed cohort? An open cohort? • What is the denominator in a cohort study? • How is it calculated?
Elements of longitudinal study designsEssential question: what is the nature of time? Confounding Modification Mediation Changes in exposures Exposures At start of study History of exposures Outcome(s) Exposures times Study times Study times
Longitudinal studies are all about change over time • Change in level and effects of risk factors due to • Physiological changes related (perhaps) to age • Selective survival – • Differential due to higher mortality in high risk • Competing risk from other outcomes (esp death) • Differential attrition by exposure • Biasing effects of attrition • Time trends in population levels of exposure • Reverse causality of disease on exposure • Proximity of exposure measurement to outcome
Factors determining trends with age in risk factor–disease associations Kaplan & Haan 1999
Change over time in risk-factor disease associations Kaplan & Haan
What is the consequence for effect estimates of misclassifying exposure time? Classifying person time exposed
Estimating exposure over time • Measurement of exposure (validity, reliability) • Change over time in exposure • Baseline • After baseline • Time that is unexposed • baseline time, average over time, cumulative exposure
Time exposed vs. time at risk • Time from exposure to event • Induction period • Threshold of cumulative exposure • Average exposure, cumulative exposure, • Immortal person time (?) • Reverse causality
The 32-year relationship between cholesterol and dementia from midlife to late life Background: Cellular and animal studies suggest that hypercholesterolemia contributes to Alzheimer disease (AD). However, the relationship between cholesterol and dementia at the population level is less clear and may vary over the lifespan. Methods: The Prospective Population Study of Women, consisting of 1,462 women without dementia aged 38–60 years, was initiated in 1968–1969 in Gothenburg, Sweden. Follow-ups were conducted in 1974–1975, 1980–1981, 1992–1993, and 2000–2001. All-cause dementia was diagnosed according to DSM-III-R criteria and AD according to National Institute of Neurological and Communicative Disorders and Stroke–Alzheimer’s Disease and Related Disorders Association criteria. Cox proportional hazards regression examined baseline, time-dependent, and change in cholesterol levels in relation to incident dementia and AD among all participants. Analyses were repeated among participants who survived to the age of 70 years or older and participated in the 2000–2001 examination. Results: Higher cholesterol level in 1968 was not associated with an increased risk of AD (highest vs lowest quartile: hazard ratio [HR] 2.82, 95% confidence interval [CI] 0.94–8.43) among those who survived to and participated in the 2000–2001 examination. While there was no association between cholesterol level and dementia when considering all participants over 32 years, a time dependent decrease in cholesterol over the follow-up was associated with an increased risk of dementia (HR 2.35, 95% CI 1.22–4.58). Conclusion: These data suggest that midlife cholesterol level is not associated with an increased risk of AD. However, there may be a slight risk among those surviving to an age at risk for dementia. Declining cholesterol levels from midlife to late life may better predict AD risk than levels obtained at one time point prior to dementia onset. Analytic strategies examining this and other risk factors across the lifespan may affect interpretation of results. Mielke et al in Neurology® 2010;75:1888–1895
Fig 1 - Mean cholesterol levels in the Prospective Population Study of Women by examination year andbirth cohort
Table 1 Characteristics of PPSW participants by dementia status over 32years (n 1,462)
General Definition of a Case-Control Study A method of sampling a population in which cases of disease are identified and enrolled, and a sample of non-cases of the population that produced the cases is identified and enrolled. Exposures are determined in the same way for individuals in each group.
“TROHOC” (cohort) STUDIES • This disparaging term was given to case-control studies because their logic seemed backwards and they seemed more prone to bias than other designs. • No basis for this derogation. • Case-control studies are a logical extension of cohort studies and an efficient way to learn about associations.
Introduction • Hypo. Example: Vitamin D exposure increases the risk of breast cancer. • Consider a hypothetical prospective cohort study of 89,949 women aged 34-59; 1,439 breast cancer cases identified over 8 years of follow-up • Blood drawn on all at beginning of follow-up and frozen • Exposure: Level of Vit D in blood characterized as high or low
Breast Cancer Results Vit D
Practical Problem: Quantifying Vit D levels in the blood is very expensive -- it's not practical to analyze all 89,949 blood samples To be efficient, analyze blood on all cases (N=1,439) but just take a sample of the women who did not get breast cancer, say two times as many cases (N=2,878)
All cases and subsample of controls Breast Cancer Vit D These data can be used to estimate the relative risk. • Identify cases of disease from a defined population, • take a sample of controls from that population.
When is it a good idea to conduct a case-control study? • When exposure data are expensive or difficult to obtain - Ex: Vit D study described earlier • When disease has long induction and latent period - Ex: Cancer, cardiovascular disease • When the disease is rare • Ex: Studying risk factors for birth defects • When little is known about the disease • Ex. Early studies of AIDS • When underlying population is dynamic • Ex: Studying breast cancer on Cape Cod
Cases • Criteria for case definition should lead to accurate classification of disease • Efficient and accurate sources should be used to identify cases: eg, existing registries, hospitals Disease Exposed
Cases give you the numerators of the rates of disease in exposed and unexposed groups being compared: • Rate of disease in exposed: a/? • Rate of disease in unexposed: c/? The denominators are missing. If this were a cohort study, you would have the total population (if you were calculating cumulative incidence) or total person-years (if you were calculating incidence rates) for both the exposed and non exposed groups, which would provide the denominators for the compared rates.
Where do you get the information for the denominators in a case control study? THE CONTROLS. • A case-control study can be considered a less costly, more efficient form of a cohort study. • Cases are the same as those that would be included in a cohort study. • Controls provide a fast and inexpensive means of obtaining the exposure experience in the population that gave rise to the cases.
Controls • Definition: A subsample of the source population that gave rise to the cases. • Ideal: nested case-control study from a cohort • Purpose: To compare the exposure distribution in the source population that produced the cases.
Selecting Controls • General population controls • Existing cohort study • Most often used when cases are selected from a defined geographic population • Sources: random digit dialing, residence lists, drivers’ license records
Selecting Controls Advantages of general population or cohort study controls: Because of selection process, investigator is usually assured that they come from the same base population as the cases. In a cohort, exposure is standardized for both cases and controls
Selecting Controls Disadvantages of general population controls Time consuming, expensive, hard to contact and get cooperation; may remember exposures differently than cases (recall bias)
Selecting Controls Hospital controls • Used most often when cases are selected from a hospital population Example: Study of cigarette smoking and myocardial infarction among women. Cases identified from admissions to hospital coronary care units. Controls drawn from surgical, orthopedic, and medical unit of same hospital. Controls included patients with musculoskeletal and abdominal disease, trauma, and other non-coronary conditions.
Advantages of hospital controls • Same selection factors that led cases to hospital led controls to hospital (?) • Easily identifiable and accessible (so less expensive than population-based controls) • Accuracy of exposure recall comparable to that of cases since controls are also sick (?) • More willing to participate than population-based controls
Disadvantages of hospital controls • Since hospital based controls are ill, they are unlikely to accurately represent the exposure history in the population that produced the cases • Hospital catchment areas may be different for different diseases
What illnesses make good hospital controls? Those illnesses that have no relation to the risk factor(s) under study Q : Should respiratory diseases be used as controls for a study of smoking and myocardial infarction? Do they represent the distribution of smoking in the entire population that gave rise to the cases of MI?
Selecting Controls Special control groups like friends, spouses, siblings, and deceased individuals. • These special controls are rarely used. • Exposures in these controls may not be independent of cases, eg, diet in families. What effect would that have on the estimate? • Some cases are not able to nominate controls because they have few appropriate friends, are widowed, or are only or adopted children. • Dead controls are tricky to use because they are more likely than living controls to smoke and drink.
Sampling a cohort population for controls: nested case-control study 1. Sample the population at risk at the start of the observation period *-------------------------------------------------------------------------* Start FU End FU ^^
Sampling a cohort population for controls: nested case-control study 2. Sample population at risk as cases develop *-------------------------------------------------------------------------* Start FU End FU ^ ^ ^ ^^^ ^
Sampling a cohort population for controls: nested case-control study 3. Sample survivors at the end of the observation period *------------------------------------------------------------------------* Start FU End FU ^^
Nested case-control study on Vit D and breast cancer Hypothetical cohort study of 89,949 women; 1,439 breast cancer cases identified over 8 years of follow-up Blood drawn on all 89,949 at beginning of follow-up and frozen Exposure: Level of Vit D in blood characterized as high or low
Nested case-control study on Vit D and breast cancer Breast Cancer Vit D Analyzed blood on all cases (N=1,439) and a sample of controls (N=2,878 – 3.3% of non cases).
Analysis of case-control studies Exposed Because controls are a sample of the population that produced the cases, size of the total population may be unknown.
Analysis of case-control studies • Two possible outcomes for an exposed person: case or not Odds=a/b • Two possible outcomes for an unexposed person: case or not Odds=c/d Odds ratio = odds of an exposed person being a case = a/b = ad/bc odds of unexposed person being a case c/d • Just like the incidence rate ratio and cumulative incidence ratio, the odds ratio is a ratio measure of association.
Analysis of case-control studies EXAMPLE: Case control study of spontaneous abortion and prior induced abortion (OUTCOME = spontaneous abortion; EXPOSURE = prior induced abortion)
Analysis of case-control studies • Odds of being a case among the exposed = 42/247 (a/b) • Odds of being a case among the unexposed = 107/825 (c/d) • Odds ratio = [(a/b) / (c/d)] = [(42/247) / (107/825)] = 1.31 Women with a history of induced abortion had a 30% increased risk of having a spontaneous abortion compared to women who never had an induced abortion.
Strengths of case-control studies • Efficient for rare diseases and diseases with long induction and latent period. • Can evaluate many risk factors for the same disease. So, good for diseases about which little is known.
Weaknesses of case-control studies • Inefficient for rare exposures • Vulnerable to bias because of retrospective nature of study • May have poor information on exposure because retrospective • Difficult to infer temporal relationship between exposure and disease How do these strengths and weaknesses compare to cohort studies?