Download
1 / 29
300 likes | 707 Vues
Diabetes and the foot. What is happening and how to treat it Helen Moakes Specialist Diabetes Podiatrist. Overview. National Guidelines and Statistics Diabetes annual foot review – the foot assessment How do problems start? Types of diabetic foot Acute foot problems Charcot foot

E N D
Diabetes and the foot What is happening and how to treat it Helen Moakes Specialist Diabetes Podiatrist
Overview National Guidelines and Statistics Diabetes annual foot review – the foot assessment How do problems start? Types of diabetic foot Acute foot problems Charcot foot What to do with them!
National Guidelines • NICE CG10 – Prevention and Management of Foot Problems in Type 2 Diabetes • NICE CG119 – Inpatient Management of Diabetic Foot Problems • Putting Feet First – NHS Diabetes • National Minimum Skills Framework for Commissioning of Foot Care Services for People with Diabetes • NSF Diabetes – DoH document
National Statistics(Putting Feet First and Fast – NHS Diabetes summary doc) • 1 in 7 people with diabetes will develop a foot ulcer • 1 in 12 ulcers results in an amputation • 8-10% of inpatients have a pressure sore and 50% of these have diabetes • 25% of diabetic patients are admitted to hospital with foot ulceration as primary diagnosis • Direct relationship between the time to healing and the time to assessment
National Statistics(Putting Feet First National Skills Framework – NHS Diabetes) • 70 amputations per week, of which 80% are potentially preventable • In 2007/2008 nearly a quarter (23 per cent) of people did not have a foot check • Diabetes complications of the foot estimated to account for 20% of total cost of diabetes care in UK
Foot Assessment • On newly diagnosed patients and annually thereafter • Identifies risk factors (neuropathy, ischaemia, deformity, previous ulceration, smoking, poor glucose control, callosities) • Assessment will result in a Risk Classification or Status – QOF indicator DM29 • Risk classification informs education needs and further care planning
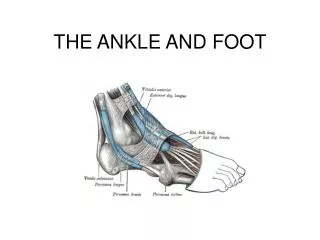
Foot Assessment What to check? Foot pulses (Dorsalis Pedis & Posterior Tibial) • Check by hand • Doppler if unable to palpate • Oedema • Also an indicator of vascular problems elsewhere
Foot assessment continued • What to check? • Protective pain sensation (neuropathy) • - 10g Monofilament (Bailey/Owen Mumford) • - Test sites • - Tell patient result! • Diagnosis of neuropathy means greatly increased chance of developing foot ulcer due to inability to sense pain
What else? • When undertaking the diabetes foot assessment, look at: • Foot shape • Deformity • Footwear • Smoking • Glucose control • Callosities • Risk status – NICE guidelines and QOF
Risk Classification(NICE guideline CG10, QOF indicator DM29 • Low Risk • - Normal sensation, palpable pulses • Increased Risk or At Risk • - Neuropathy OR absent pulses • High Risk • - Neuropathy AND/OR absent pulses AND pathology • Ulcerated foot
How do problems start? • High blood glucose levels • Start of damage to nerves and blood vessels • Diabetes may not be diagnosed • Once diagnosed, poor control of BG levels • Lack of education and knowledge • Fear • Injury/trauma • Painless! • Ischaemia - pain • Painful neuropathy • Amputations
Types of Diabetic Foot • Neuropathic • Pink and warm • Good pulses • Abnormal monofilament result • Dry • Callus • High arch, claw toes • Neuro-ischaemic • Dusky/Blueish and cool/cold • Non-palpable pulses • Abnormal monofilament (?) • Little callus, glassy • Pain
Neuropathic Feet(typical features) • Common • Look ‘normal’ • Education of paramount importance • Protection – footwear, insoles, not barefoot! • Podiatry care if required – varies with area • BG control • Painful neuropathy • Swift referral
Neuro-Ischaemic Feet (typical features) • Less common • Fragile • Life expectancy reduced • Often painful • Poor healing • Protection essential to prevent injury/trauma • Podiatry care • Swift referral
INFECTION IS A KILLER OF DIABETIC FEET Don’t leave it! Find out your nearest hospital Foot Clinic contact details
Acute Foot Problems • Assess urgency (pyrexic, BG level, wound) • Get a history • Will almost always require referral to Foot Clinic • Often requires admission • If unsure, get advice
Acute Foot Problems – possible examples • Blisters • Callus with tissue breakdown underneath • Ingrowing toenail • Accidental trauma – stubbing toe, cuts/grazes • ANYTHING INFECTED
Charcot foot • Process affecting the bony structure of the feet • Rare but under-diagnosed • Affects neuropaths with good blood supply • Diagnosis difficult – differentials?
Charcot foot – the process • Neuropathic – insensate • Bones within foot/ankle soften due to arterio-venous shunting • Bounding foot pulses • TRAUMA ?? • Bones begin to fracture within foot/ankle • Foot may swell, redden, increased temperature • Mostly unilateral, 20% bilateral involvement • Pain/discomfort?? • Foot/ankle changes shape (collapse/rocker bottom) ...but we can avoid this...
Charcot foot - diagnosis • REFER TO FOOT CLINIC • X-ray – not as useful in early stages but gives a baseline • Bone scan – detects heat • HbA1c, Hb, ESR & CRP • Rule out infection, DVT, etc
Charcot Foot - treatment • TOTAL CONTACT PLASTER CAST – gold standard • Time in cast varies – couple of months to 18 months • Transition to Aircast, then custom footwear • Can take 3 years • Prevent by good BG control, lessen complications, education
What to Do! • If in doubt with any diabetic foot problem... SEEK ADVICE.......FAST! • Hospital MDT foot clinics are there to help • Diabetic feet can deteriorate fast, especially with infection • Prevention is key
Thank you! Any Questions?