Download
1 / 28
280 likes | 402 Vues
Cultural Sensitivity and Cancer Patients. Darryl L. Jordan, M.D. Assistant Professor Liaison Medical Director for Veteran Affairs at Meharry. Disclaimer.

E N D
Cultural Sensitivity and Cancer Patients Darryl L. Jordan, M.D. Assistant Professor Liaison Medical Director for Veteran Affairs at Meharry
Disclaimer In accordance with accreditation counsel for continuing medical education (ACCME) guidelines, I disclosed that I have no financial relationship with any pharmaceutical or medical manufacturing companies that would pose a conflict of interest to this presentation.
Objectives • Review variation in cancer mortality rates among various populations via socio- demographic factors • Identify barriers to cancer assessment and treatment of underserved minority populations • Review program designed to eliminating health disparities
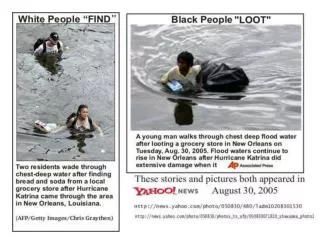
Summary Statement of the American Cancer Society1989: Cancer in the Poor Findings 1. Poor people endure greater pain an suffering from cancer than other Americans 2. Poor people and their families must make extraordinary personal sacrifices to obtain and pay for care. 3. Poor people face substantial obstacles in obtaining and using health insurance and often do not seek care if they cannot pay for it. 4. Current cancer education programs are culturally insensitive and irrelevant to many poor people. 5. Fatalism about cancer is prevalentamong the poor and prevents them from seeking care.
Summary Statement of the American Cancer Society1989: Cancer in the Poor Challenges for the Nation Establish patient advocate and referral services to help poor patients navigate the health system and manage personal problems that result from cancer treatment. Involve community organizations serving the poor and poor people themselves in cancer education and patient advocacy programs.
Patient Navigator Outreach and Chronic Disease Prevention Act of 2005 Requires the Secretary of Health and Human Services acting through the Administrator of the Health Resources and Services Adminstration (HRSA) to make grants to eligible entities for the development and operation of demonstration programs to provide patient navigotor services to improve health care outcomes. Requires the Secretary to coordinate with, and ensure the participation of, the Indian Health Service, the National Cancer Institute, and of the Office of Rural Health Policy..
Reasons for Cancer Disparities Environment Social and Systemic Factors Genetics Biology/ Patient \Tumor Factors Lifestyle Behavioral/Patient Factors Gabram S et. Al Cancer 2008
Impact of Socioeconomic Status on Survival after Cancer in the U.S Method: Review of medical records, diagnosis stage, treatment and 5-yr mortality and SES, across 7 cancer registries within the U.S. from 1996-1997 4,844 women with breast cancer 4332 men with prostate cancer 4422 men and women with colorectal cancer Results: For all 3 cancer sites, low SES was a much stronger predictor of mortality among individuals aged < 65 yrs and among individuals from racial/ethnic minority groups. Byers et. Al Cancer 2008
Impact of Socioeconomic Status on Survival after Cancer in the U.S Conclusion: The current results indicate that low SES is a risk factor for all-cause mortality after a diagnosis of cancer. These findings support the need to focus on SES as an underlying factor in cancer disparities by race and ethnicity. Byers et. Al Cancer 2008
Effects of an outreach and internal navigation program on Breast cancer diagnosis in an urban cancer center with a large African-American population Method: Cross-sectional study was an analysis of all women with breast cancer who were diagnosed and/or treated 2001 and 2004 intervention with 125 community health advocates (CHAs), educational programs and Patient Navigators communicated directly with patients to encourage screening, diagnostic procedures and treatment. Results: 487 patients were diagnosed/treated from 2001 and 2004 with 1148 community interventions by CHAs with est. > 10,000 participants, proportion ofstage 0 ( in situ ) breast cancers increased from12.4% to 25.8% stage IVinvasive breast cancer declined from16.8% to 9.4% Grabam S et. Al Cancer 2008
Effects of an outreach and internal navigation program on Breast cancer diagnosis in an urban cancer center with a large African-American population Conclusions: The outreach initiatives and internal patient navigation appear to have improved stage at diagnosis. Similarly, prospective data are being collected to determine whether Patient Navigators influence treatment and appointment adherence as well as the underlying reasons for barriers to specific interventions in this underserved minority population. Grabam S et. Al Cancer 2008
Racial Differences Pertaining to a Belief about Lung Cancer SurgeryResults of a Multicenter SurveyMitchell L. Margolis, MD; Jason D. Christie, MD, MS; Gerard A. Silvestri, MD; Larry Kaiser, MD; Silverio Santiago, MD;and John Hansen-Flaschen, MD Objective: To assess the prevalence of the belief that air exposure during lung cancer surgery might cause tumor spread Setting: Philadelphia VAMC, Los Angeles VAMC and Medical University of South Carolina Patients: 626 consecutive patients in pulmonary and lung cancer clinics Ann Intern Med 2003; 139:558-563
Results: 38% of patients 61% of whom were AA and 29% whom were Caucasians) stated that they believed air exposure at surgery causes tumor spread; 19% of AA stated that they would oppose surgery because of this belief. 14% would not accept their physicians assertion that the belief was false. Ann Intern Med 2003; 139:558-563
Conclusion: Belief in accelerated tumor spread at surgery is prevalent among pulmonary outpatients and lung cancer patients facing lung surgery, particularly African Americans. This finding may pertain to key racial disparities in lung cancer. Ann Intern Med 2003; 139:558-563
Founder of Navigational Approach 1989 American Cancer Society, Report to the Nation Cancer in the Poor 2005 Patient Navigator Outreach and Chronic Disease Prevention Act June 2007 Harold P. Freeman Patient Navigation Institute opened Harold P Freeman, M.D. Associate Director of NCI Director of the NCI Center to Reduce Cancer Health Disparities
Conclusion Socio-economic factors and cultural sensitive play a important role in health disparities among minority populations Patient Navigator programs have proven benefit in reducing the impact of health disparities Additional studies are need to evaluate the financial impact of such programs on future health care cost
References Byers T, Wolf H, Bauer K, Bolick-Aldrich S, The Impact of Socioeconomic Status on Survival After Cancer in the United States, Cancer 2008;113; 582-590. Gabram S, Lund M, Gardner J, Hatchett N, Effects of an Outreach and Internal Navigation Program on Breast Cancer Diagnosis in an Urban Cancer Center With a Large African-American Population, Cancer 2008; 113; 602-607. Margolis M, Christie J.D., Silvestri G, Kaiser L., Santigo S., Hansen-Flaschen J, Annual of Internal Medicine 2003: 139; 558-563