Pulmonary Ventilation
Pulmonary Ventilation. Week 2 Dr. Walid Daoud A. Professor. Pulmonary Ventilation. Pulmonary ventilation is mass movement of air in and out of the lungs. Forces for Pulmonary Ventilation: Pressure gradient between alveoli and atmosphere.

Pulmonary Ventilation
E N D
Presentation Transcript
Pulmonary Ventilation Week 2 Dr. Walid Daoud A. Professor
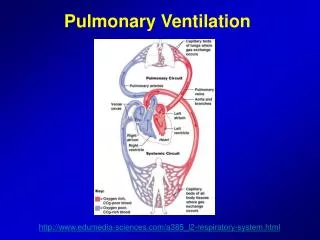
Pulmonary Ventilation Pulmonary ventilation is mass movement of air in and out of the lungs. Forces for Pulmonary Ventilation: Pressure gradient between alveoli and atmosphere. Inspiration occurs when pressure in atmosphere exceeds pressure in alveoli.
Intra-alveolar Pressure At sea level, atm. pressure is 760 mmHg and all pressures in the respiratory system are expressed relative to atmospheric pressure. -During inspiration Palv. = - 1 mmHg -During expiration Palv. = + 1 mmHg -At ends of inspiration & expiration= 0 mmHg Changes in intra-alveolar pressure are caused by changes in volumes of lungs.
Intra-pleural Pressure It is the pressure inside pleural space. It is always negative under normal conditions. . At end of normal expiration= - 4 mmHg . At end of normal inspiration= -6 to -8 mmHg . During forced inpiration with glottis closed = - 30 to - 40 mmHg (Muller experiment). . During forced expiration with glottis closed = + 50 mmHg (Valsalva experiment).
Importance of negative intra-pleural pressure - It helps lung expansion. - It helps venous and lymphatic return to the heart. - It is a measure of lung elasticity (recoil pressure).
Transpulmonary Pressure It is difference between intralveolar and intrapleural pressures. = Palv. – Ppl = 0 – (-4 ) = 4 mmHg Transpulmonary pressure is called distending pressure which is the force acting to expand the lung against elastic recoil of the stretched lung.
Causes of Negative Intrapleural pressure The negativity is due to continuous tendency of lungs to recoil inward against continuous tendency of chest wall to expand outward to reach their relaxation volume. Causes of recoil tendency of lungs: 1- Elastic tissues of lungs 2- Surface tension of fluid lining the alveoli.
Pulmonary Surfactant A detergent -like substance secreted by type II alveolar cells. Nature: Complex mixture of phospholipid dipalmitoyl lecithin, apoproteins and calcium ions. Functions: - Facilitation of lung expansion. - Prevention of alveolar collapse during exp. - Prevention of pulmonary edema.
Surfactant Deficiency 1- Respiratory distress syndrome (RDS). 2- Long-term inhalation of 100% oxygen. 3- Occlusion of one pulmonary artery. 4- Cigarette smoking. 5- Hypothyroidism. 6- Hypocoticism. 7- Hyperinsulinism.
Mechanism of Respiration . Inspiration. Active process. . Expiration. Resting expiration is a passive process while forced expiration is an active one.
Spirometry Spirometer Itis a device to measure lung volumes and capacities. Spirometry Itis the used technique . Spirogram Itis the recording.
Pulmonary Volumes 1- Tidal volume (VT). 2- Inspiratory reserve volume (IRV). 3- Expiratory reserve volume (ERV). 4- Residual volume (RV). RV can not be measured by spirometry but can be calculated by helium-dilution method.
Pulmonary Capacities 1- Inspiratory capacity (IC). 2- Vital capacity (VC). 3- Functional residual capacity (FRC). 4- Total lung capacity (TLC). FRC and TLC can not be measured by spirometry.
Factors affecting vital capacity Physiological variations: 1- VC increases in: Males, athletes and standing position. 2- VC decreases in: Females, pregnancy and recumbent position.
Factors affecting vital capacity Clinical significance of VC: VC is an index of lung function and strength of respiratory muscles: 1- Paralysis or myositis of resp. muscles. 2- Bone deformities e.g, kyphosis or scoliosis. 3- Loss of lung elasticity e.g, emphysema. 4- Restrictive lung diseases e.g, lung fibrosis. 5- Obstructive lung diseases e.g, asthma. 6- Abdominal tumors.
Timed Vital capacity - Forced expiratory volume in first second (FEV1). - Forced vital capacity (FVC). Normally FEV1 = 80% of FVC In diseases: -Restrictive lung diseases: lung fibrosis: . Both FEV1 & FVC are reduced. . FEV1/FVC % is normal. -Obstructive lung diseases: brochial asthma. . FEV1 is reduced more than FVC . FEV1/FVC % is low.