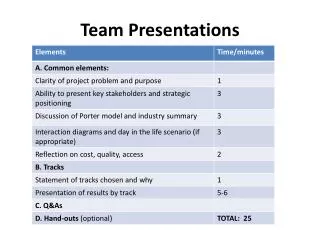

Team Presentations
E N D
Presentation Transcript
Team Presentations Felicity Topp and Rochelle Condon 5TH October 2004
Concurrent Session 1Team Presentations Bellarine Room 1 • Ballarat Health Service • Goulburn Valley Health • Western Health • Royal Children's Hospital
Patient Flow Collaborative Fiona Brew Phil Catterson Jill O’Flynn Operating Suite Emergency Department PDU Ballarat Health Services- ‘The Stream Team’
Summarise Organisational Constraint areas BHS Constraint Background • Culture • Stable workforce • Education level • Flexibility • History • Medically driven organisation • VMO mentality • Public v Private • Opportunity • Current practice - ? Good / Bad / Ugly • Cascade effect - isolation / up and downstream impact
Summarise Priority Constraint Area 1 System Approach - Access to Theatre • Timing of cases • am vs pm - length of stay • Session allocation • emergency • elective • Delays • entry • exit
Diagnostic work • Process • Staff Involved • Nursing, Medical, Support • Staff Reaction • Keen, positive • Useful data • Tally charts
Improvement Plan • Action Plan • tally chart presentation • champion selection • Strategies developed • Identify Culture • Paddle own canoe • Going with the flow • Aiming for improved stream? • Communication • Work practices • Roles • Most work in daylight hours • Utilise DOSA unit
Progress • Communication • Centralised distribution • Culture • Patient focus • Team approach - New skills • Planning • Work practices • Roles • Day surgery focus
Lessons learnt • Success • Communication • Culture • avoid isolation • Work processes / practices • strategies embedded in culture • Future Improvements • Education • Frequency • One size does not fit all
Desired Impact • Recognition of cascade effect • impact on patient flow • global view • Action • purposeful • innovative • positive - up and downstream validation prior • Evaluation • patient perspective
Next Steps • Consolidation • Increased medical ‘buy in’ • Feedback • Further development of strategies • outcomes related to measures
Patient Flow Collaborative Kim ReadGoulburn Valley Health
Summarise Organisational Constraint areas • Of the 5 Major constraints @ GVH, 2 constraint areas were prioritised due to the current internal efforts/projects being undertaken to improve patient flow: • 1. Major Bowel Surgery Admissions • 2. Discharge Planning/Communication
Summarise Priority Constraint Area 1 • Bed Availability. • Major Bowel Surgery Admissions on day prior. • What works for us and OUR PATIENTS.
Diagnostic work • Day of Surgery Admission (DOSA)rates • Patient Interviews • Staff Interviews • Process Mapping
Patient Interviews • First Patient • Noted what seemed to be a long wait to be seen by specialist after referral. • Had support of wife and daughter when making decision to go ahead with surgery. Glad of their presence during discussions. • Noted the effort to get surgery done in short period of time once decision made. • Had bowel preparation in hospital but would have been happy to have this in his own home environment. • Pain relief post operatively was good. • Felt he started solids too soon after – vomiting and subsequent naso-gastric tube. • All went well after discharge and for follow up. • Second Patient • Felt that all went quickly in relation to being seen and being booked for surgery. • Was distressed and horrified with diagnosis and need for subsequent surgery. • Younger female patient who requested to have bowel preparation at home. • Discussed at pre-admission clinic her desire to be at home with her husband pre-operatively. Wanted to be in thecomfort of her own home, and in her own bed. Although she had nausea with the bowel preparation, she would not change her mind about having the prep at home. • Discussed problems with pain relief post-operatively. • Had problems after discharge with nausea and became dehydrated. • Required representation to Emergency Department for re-hydration and issues related to the drain tube.
Improvement Plan • Research bowel preparation options. • Surgeon Involvement. • Research processes at other institutions. • Relationship with private hospital.
Progress • Proposed process map. • Commenced clinical guideline. • Motel Accommodation guideline.
Lessons learnt • One bite at a time. • Involve the key players. • Has to make a positive difference for all.
Desired Impact • Satisfactory preparation. • Patient’s needs met. • Bed availability (HIPs). • DOSA rates comparable.
Summarise Priority Constraint Area 2 • Discharge Planning/Communication • potential improvement option • Poor performance of discharge planning & communication linked to lack of bed availability • potential increased unplanned re-admission rates
Diagnostic work • Satisfaction Surveys/Medical File Audits(R1) • Patients/Service Providers/Clinical Staff(R2) • Staff lackunderstanding of effective discharge planning and further hindered by lack of appropriate risk assessment tools+lengthy & complicated referral forms/systems. • Random Patient Satisfaction Survey(R3) • Patient thoughts/feelings/perception of self-care needs. • Patient lack of understanding & misconception about current day healthcare environment (e.g > LOS)
Improvement Plan • Review & re-development of pre-admission/emergency admission documentation • Implementation of streamlined internal referral. • Review & re-development of discharge summary (R4) • Development of decision support tools-D/P(R5) • Development of Clinical Practice Guidelines-Admission & Discharge
Progress • Improvement strategies gathering momentum • Improved awareness of the importance of discharge planning at day 1 of admission to support clinical outcomes (R5.2) • New Referral System + Discharge Summary dissemination system(R6) - Included patients admitted from March 2004 • Included all clinical staff (acute/sub-acute & ED)
Lessons learnt • System change alone will fail unless supported by culture change, which in turn is supported by effective education and communication support strategies. • Referral system development- would repeat consultation process. • Development of new admission/assessment documentation taking longer that envisaged due to complicated consultation process and variety of internal/external influences • Discharge Summary review-would include internal satisfaction review and corresponding time with GP satisfaction review
Desired Impact • Improved patient and carer satisfaction with the discharge process and health outcomes. • Services will be integrated across the continuum of care. • Length of stay will be comparable to industry benchmarks. • Reduction in rate of unplanned readmissions within 28 days of initial separation. • Improved processes of transition across the acute, sub-acute and community interfaces
Next Steps • Continue development of streamlined admission,health assessment & risk screen documentation to improve patient assessment consistency and early identification/intervention • Ongoing education and support for staff regarding D/P- empower ALL STAFF to be skilled in D/P to improve patient journey thru healthcare continuum
Patient Flow Collaborative General Internal Medicine UnitWestern Hospital, FootscrayG. Lane, Head of UnitH. Hasanoglu, NUM
Background: General Internal Medicine UnitPatient Mix • Daily average of 45 inpatients (range 25 to 90) • Average age 79 years • Varied ethnic backgrounds • Several acute medical problems • Scarcity of community support or supportive accommodation
Cardiac failure Ischaemic heart disease Cognitive impairment Falls Urinary tract sepsis Septicaemia Pneumonia Unstable diabetes Acute and chronic renal impairment Polypharmacy problems Syncope Obstructive lung disease Psychiatric diagnoses Self-harm Accommodation and community support problems Background: General Internal Medicine Unit. Common Problems
Diagnostic work: A • 2 week period of reporting by all junior medical and daytime nursing staff of processes which possibly delayed patient flow • Recorded daily at nursing and medical handover • Staff reactions: • Nursing: cautious enthusiasm • Medical: cautious cynicism
Diagnostic work: B • Patient Flow Profile • 3 patients tracked and interviewed throughout their admission • Most interactions with health personnel recorded, including process delays • Patients’ opinions sought about: • Being told what was wrong • Being told about my treatment • Going home • Being followed up • Felt to be less useful than “A”
Organisational Constraint areas • Delay in patients being seen for consultations and procedures was the 2nd highest rating process
Desired Impact • 50% reduction in: • mean time • range waiting for consultations and procedures • ? Significant reduction in length of stay
Measures reflecting the effect of the constraint on the organisation before and after test cycles a) Time to see patient by registrar b) Time to see patient by consultant
Pre-intervention • Days to see patient: Registrar Pre (n=27) n 18 Range 0-7 Median 0 Mean 1.2 SD 1.93 Variance 3.7
Pre-intervention • Days to see patient: Consultant Pre (n=27) n 14 Range 0-6 Median 2 Mean 1.9 SD 1.89 Variance 3.6
How Improvement Strategies were derived and implemented • Discussion with General Internal Medicine Unit staff (junior and senior) about reasons for delays in consultations and procedures • Consensus on the most practical intervention strategy
Improvement Strategy Change to referral process: If registrar of other unit had not seen the patient by the next day, the parent unit consultant would contact the consultant of the other unit
Outcomes • Days to see patient: Registrar Pre (n=27) Post (n=24) n 18 19 Range 0-7 0-4 Median 0 0 Mean 1.2 0.68 SD 1.93 1.06 Variance 3.7 1.1 Not seen 9 5 by reg
Outcomes • Days to see patient: Consultant Pre (n=27) Post (n=24) n 14 9 Range 0-6 0-7 Median 2 2 Mean 1.9 2.2 SD 1.89 1.92 Variance 3.6 3.7 Not seen 13 15 by cons
Lessons learnt • Time intensive • The challenges of frequent changes in junior staff • ?Hawthorne effect • Procedures often escaped reporting • Difficult to record exact times • Too short a study time to assess whether intervention would affect overall length of stay
What would you now do differently? • Focus on delay to procedures rather than consultations • Devise an electronic collection process of data by Unit’s registrars • Weekly audit of delayed procedures and consultations at Unit’s Safety and Quality meeting • Display recording sheets on all wards