Aortic regurgitation
Aortic regurgitation. Dr Husain Tayib. Aortic regurgitation. * Any conditions resulting in incompetent aortic leaflets _ Congenital Bicuspid AV _Aortopathy Cystic medial necrosis Collagen disorders (.Marfan Syn.] Ehler-Danlos

Aortic regurgitation
E N D
Presentation Transcript
Aortic regurgitation Dr Husain Tayib
*Any conditions resulting in incompetent aortic leaflets _Congenital Bicuspid AV _Aortopathy Cystic medial necrosis Collagen disorders (.Marfan Syn.] Ehler-Danlos Osteogenesis imperfecta Pseudoxanthoma elasticum _Acquired * Rheumatic heart disease *Dilated aorta [ hyperte.] *Degenerative *Connective tissue disorder _ Ankylosingspondylitis, _Rheumatoid arthritis, _Reiter’s syndrome, _Giant-cell arteritis ) *Syphilis (chronic aortitis) *Acute AR: , _Infective endocarditis, _Trauma _Dissecting aneurysm Etiology Aortic regurgitation
Aortic regurgitation Aortic Dissection Bicuspid AV Marfan syndrome
Aortic regurgitation Pathophysiology Chronic AR Elevated LV end-diastolic pressure and volume Dilatation and eccentric hypertrophy of the LV Increased stroke volume Left ventricular EF normal Gradually LV preload and afterload both increased Ultimately, adaptive measures fail. LV function deteriorates End-diastolic volume rises further (the largest heart) Myocardial ischemia Decline in forward stroke volume and EF LVDOL…. LV dilatation …. Increased SV ….. Wide PP…..LVH …Dilated LA …. Increased LVEDP……LAP rise ….. Pulmonary congestion …. PH …. RVH ……RVF
Symptoms Aortic regurgitation Mild to moderate AR : * Often asymptomatic * Palpitation Severe AR : _Dyspnea, orthopnea, PND _Chest pain. Nocturnal angina >> exertional angina { diastolic aortic pressure and increased LVEDP thus coronary artery diastolic flow} *With extreme reductions in diastolic pressures {e.g. < 40} may see angina
_Quincke’s sign: capillary pulsation _Corrigan’s sign: _Water hammer pulse _Bisferiens pulse (AS/AR > AR) _De Musset’s sign: systolic head bobbing _Mueller’s sign: systolic pulsation of uvula _Durosier’s sign: femoral retrograde bruits _Traube’s sign: pistol shot femorals _Hill’s sign:BP Lower extremity >BP Upper extremity by _> 20 mm Hg - mild AR _> 40 mm Hg – mod AR _> 60 mm Hg – severe AR Aortic regurgitation PeripheralSigns
Apex: _Enlarged _Displaced _Hyper-dynamicLforcible nonsustained _Palpable S3 _Austin-Flint murmur Aortic diastolic murmur _Length correlates with severity {chronic AR} _In acute AR murmur shortens as Aortic DP=LVEDP _In acute AR - mitral pre-closure Central Signs of Severe Aortic regurgitation
AUSCULTATION Murmur: high-pitched, blowing, decrescendo diastolic murmur, heard best in the third intercostal space along the left sternal border (holodiastolic in severe AR) When the murmur is soft, it can be heard best with the diapgm hraof the stethoscope and with the patient sitting up, leaning forward, and with the breath held in forced expiration. Aortic regurgitation Physical examination • Widened pulse pressure • systolic – diastolic = pulse pressure • _ S1 S2 S1 10
A mid-systolic ejection murmur frequently audible in isolated AR Flint murmur, a soft, low-pitched, rumbling mid-diastolic murmur probably produced by the diastolic displacement of the anterior leaflet of the mitral valve by the AR stream not due to hemodynamically significant mitral obstruction 11
Common Murmurs and Timing Aortic regurgitation ,_Systolic Murmurs _ Aortic stenosis _ Mitral insufficiency _Mitral valve prolapse _Tricuspid insufficiency Diastolic Murmurs _Aortic insufficiency _Mitral stenosis S1 S2 S1
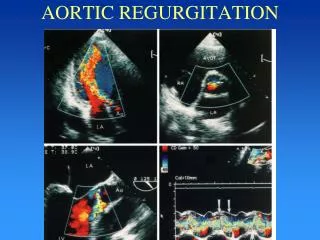
Aortic regurgitation Investigations : *ECG :- LVH + T inversion *Chest XR :- _ Cadiac dilatation _ Aortic dilatation _ Pulmonary congestion *ECHO :- _Dilated LV _ Hyperdynamic LV _Fluttering AML _ Doppler detects reflux *Cardiac Catheterization :- _Dilated LV _ AR _Dilated aortic root
Aortic regurgitation Chest XRPA view
Aortic regurgitation LVH ECG
Aortic regurgitation CW-doppler AR AR+AS CFM AR AR AR
Assessing severity of AR Aortic regurgitation *Assess severity by impact on peripheral signs and LV peripheral signs = severity LV = severity S3 Austin –Flint murmer LVH radiological cardiomegaly
Natural history : Aortic regurgitation *Asymptomatic %/Y Normal LV function {--good prognosis} _Progression to symptoms or LV dysfunction < 6 _Progression to asymptomatic LV dysfunction < 3.5 _ 5-year survival 75% <0.2 _Sudden death Abnormal LV function _Progression to cardiac symptoms 25 *Symptomatic {poor prognosis _Mortality >10% TX: Medical Surgery BEFORE LV dysfunction Bonow RO, et al, JACC. 1998;32:1486.
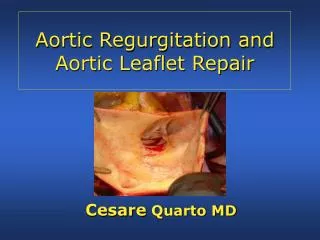
Aortic regurgitation Management : * Medical : _Vasodilator { ACEIs } _ Diuretics for pulmonary congestion _Prophylaxis against IE _Treatment of underline cause e.g. IE , Syphilis *Surgical : _AV replacement Mechanical or Bioprosthesis _Aortic root replacement for dilated A root , {e.g. Syphilis , Marfan`s syndrome , Dissecting aneurysm } *EHO indications for AVR : _LVEDD >55 _EF > 55% _FS > 27%
Criteria for Aortic Valve Replacement in Chronic Aortic Regurgitation • Symptoms Congestive heart failure. Declining exercise tolerance on exercise testing. Angina • Anatomy, regardless of symptoms: Left ventricular dysfunction: EF <50% Progressive left ventricular dilation or decline in EF on serial studies Severe dilation (echo): - Left ventricular diastolic dimension >75 mm - Left ventricular systolic dimension >55 mm -Aortic root dimension >50 mm
Aortic regurgitation AV-replacement