Download

1 / 46
680 likes | 2.14k Vues
AORTIC STENOSIS AND AORTIC REGURGITATION. PRESENTED BY: DR. Neeraj & DR. Bikash MODERATER: DR. Maya. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. AORTIC STENOSIS. Aortic valve. Normally - 3 cusps - May be bicuspid or unicuspid

E N D
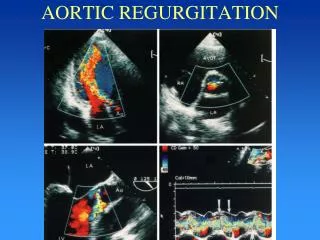
AORTIC STENOSIS AND AORTIC REGURGITATION PRESENTED BY: DR. Neeraj & DR. Bikash MODERATER: DR. Maya www.anaesthesia.co.in anaesthesia.co.in@gmail.com
Aortic valve • Normally - 3 cusps - May be bicuspid or unicuspid • Normal AV diameter =1.9 to 2.3 cm • Normal AV area= 2 - 4 cm2 (2.6 to 3.5 cm2 ) • Cusps are named according to their relation to coronary ostia - left ,right and non-coronary • Normal diameter of LVOT = 2.2 ± 0.2 cm
Incidence • ¼ of all with patient chronic VHD • Male> female (80% of adult pt with symptomatic valvular AS are male ) • It is the most common form of VHD in US
Classification • SUPRAVALVULAR VALVULAR SUBVALVULAR- Discrete Tunnel • VALVULAR – Congenital (< 30 yr) Bicuspid (40-60 yr ) Secondary to inflammation (40-60 yr ) Degenerative (>70 yr )
Etiology • Congenital- Stenotic since birth • Bicuspid – 1-2 % of population - Male > female (3 : 1 ) - 6% have coartation of aorta - Mechanical shear stress produce injury & stenosis
Cont. • Secondary to inflammation:- -Mainly rheumatic -MC cause of AS in India and world -Isolate rheumatic AS- rare (Rheumatic AS always associated with mitral valve involvement and AR ) -Post inflammation -> commissural fusion
Cont. • Degenerative:- -MC cause of AS in US and EUROPE ->30% people of >65yr –have AV sclerosis -Stenosis is due to sclerosis and calcification -Progress from the base of the cusp to the leaf-lets
Risk factors of AS • Bicuspid aortic valve • Risk factors for atherosclerosis - age - male sex - smoking - DM, HTN - ↑ LDL , ↓ HDL , ↑ CRP • Rheumatic fever • Conditions with ↑SV and altered calcium metabolism
Pathophysiology • Aortic stenosis ↓ Obstruction to LV ejection ↓ Pressure overload ↓ ↑LV mass (↑wall thickness) ↓ ← ← ← → → → ↓ ↓ Compensated Decompensated ↓LV compliance Fibrosis:↓ contractility Normal contractility ↓ ↓ LV filling ; ↓early LV dilatation ↑late ↓ ↓ SV: normal SV: decreased
Cont. • The LVH is due to increase wall tension,in accordance with Laplace”s law: Wall tension = P*R/2H p - intraventricular pressure r – inner radius h – wall thickness
Cont. Pressure overload ↓ ↑Peak systolic pressure ↓ ↑Wall tension ↓ Parallel replication of sacromeres (-) ↓ Increase wall thickness ↓ Concentric hypertrophy Concentric hypertrophy normalizes wall stress and thus preserve myocardial contractility
Cont. • Consequence of LVH – - Alternation in diastolic compliance - Imbalance in myocardial supply/demand relationship - Possible deterioration of intrinsic contractile performance of myocardium
Cont. • Pressure –volume loop in AS
Cont. • Increased chamber stiffness impedes early left ventricular filling • Hence atrial systole is critical in maintaining ventricular filling and SV • In AS atrial systole accounts for 40% of LVEDV. (Normally it contribute 15-20% of LVEDV )
Cont. • Although contractility is preserved, hypertrophied ventricle is sensitive to ischemia and LVF
Natural history • Prolonged latent period • Once moderate stenosis present rate of progression is – -0.3m/s jet velocity/yr -Mean pressure gradient= 7 mm-hg/yr -↓in valve area= 0.1cm2 /yr
Clinical presentation • Asymptomatic with ES murmur • Classical triad (angina, dyspnea, syncope ) • Sudden death (without symptoms it is <1% )
Symptoms/signs - Angina -Syncope -CHF Life expectancy 5 yr 2-3 yr 1-2 yr Cont.
Physical findings • Delayed sustain peak of arterial pulse (pulsus parvus et tardus ) • Bifid apical LV impulse • Systolic thrill • Late peaking SE murmur (2nd right intercostsl space ) • Paradoxical S2 • S4 (with LVH ) & S3 (with LVF ) (Thrill and intensity of murmur does not correlate with severity )
Investigation • CXR and ECG - LVH - Dilatation of ascending aorta - Aortic calcification
Echocardiography • 2D/Doppler TTE- test of choice • Provide information about- - Etiology, location - Valve gradient and area - Systolic/diastolic LV function - Concomitant RWMA - Coartation associated with bicuspid valve
Cardiac Catheterization • Provide information about - Pressure gradient - AVA - Cardiac output
Cont. • Gradient across valve normal until orifice area reaches less than half of normal • Onset of symptoms • 0.9 cm2 with CAD • 0.7 cm2 without CAD
Risk assessment • Increased peri and postoperative risk depend on both patient-related and procedure related factor. • AS is MC VHD in elderly -2 to 9% of adult who are >65 yr are affected by AS • Stewart et al and Lindoos et al – patients with severe AS face a17.3 % risk of cardiac complication and 13% mortality rate during non-cardiac surgery. ( j.am coll cardiology)
Cont. • Adverse perioperative risk in patient with AS depends:- - Severity of AS - Presence of concomitant CAD -Severity of surgical procedure -50% of patient with AS and angina have CAD , - Patient <40 yr with AS , with no chest pain and no coronary risk factor ,prevalence of CAD is 3-5 % ( Bonow et al,J Heart Valve Dis,1998;7 )
How to deal with healthy patient with AS facing noncardiac surgery • Medical history and physical examination= cornerstone of preoperative evaluation • According to Michael et al – (Chest 2005;128,2944-2953 )
Cont. • Non cardiac surgery can be safely performed 3 months after CABG with an cardiac risk reduction from 3.3 to 1.7 % (Anesth Analg 2002:94,) • But paucity of data for timing of valve replacement prior to elective noncardiac surgery
Role of echo and cardiac catheterization • Current recommendation:- TTE should be performed in every patient with suspected AS • Cardiac catheterization→ no extra role and is replaced by TTE. • It is now performed:- -When coronary angiography is required - There is any doubt in echo. (mochizuki et al., curr opin cardiol; 2003/18)
Management of anesthesia in AS • Anesthetic goal = avoidance of event that may further decrease CO - Maintain normal sinus rhythm - Avoid Brady and tachycardia - Avoid sudden ↓ or ↑ in SVR - Fluid management to maintain venous return and LV filling
Cont. • Premedication : - Adequate premedication to decrease undue preoperative excitement and tachycardia - Supplemental oxygen - Antibiotic prophylaxis
Monitoring • Routine monitoring • Standard 5 lead ECG v4 and v5 for ischemia lead II for arrhythmia • Use of intraoperative TEE is desirable :-value is currently undetermined
Cont. • Invasive hemodynamic monitoring is :- Controversial - Intra-arterial BP monitoring is desirable - CVP = poor estimate of LV filling when compliance is reduced - Risk with PAC is arrhythmia induced hypotension or ischemia - But PAC also allow for measurement of CO, SVO2 and possible trans-venous pacing when needed
Cont. • Induction - Few studies - But in severe AS narcotic based induction should be preferred - Preferred non-narcotic induction is by etomidate • LMA should be preferred over ETT whenever possible
Cont. • Maintenance: -In severe AS many prefer pure narcotic technique -In mild- moderate AS inhalational agents can be safely used disadvantage :-negative inotrophy -risk of arrhythmia -Although N2O has potential of ↑SVR discussion regarding this is less critical
Cont. • Intra-op hypertension and tachycardia:- - ↑ conc. Inhalational agent - If B blocker- esmolol is preferred - Temptation to control intra-op hypertension with vasodilators should be resisted (Kaplan's ) • Intra-op hypotension:- - Regardless of cause treat with alpha-agonist - Then address underline etiology (Kaplan's)
Regional anesthesia and AS • Regional anesthesia decreases SVR ,hence not preferred over GA. • Epidural is preferred over spinal • Mild-moderate AS: can tolerate spinal and epidural Severe AS: spinal and epidural are contraindicated (stoelting coexisting diseases )
Cont. • Collard et al: - Continuous spinal (.25 % bupivacain ) - 2 patients - Sever AS - Hip surgery - Invasive monitoring (Anesth.analg 1995;85)
THANK YOU www.anaesthesia.co.in anaesthesia.co.in@gmail.com