Download

1 / 82
1.16k likes | 4.05k Vues
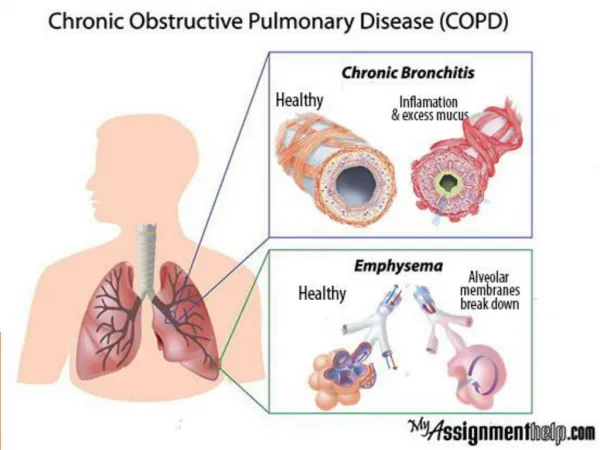
Chronic Obstructive Pulmonary Disease (COPD). A process characterized by the presence of chronic bronchitis, emphysema, or both, leading to the development of airway obstruction. What is COPD?. What is COPD?. COPD is a serious lung disease that makes it hard to breathe.

E N D
Chronic Obstructive Pulmonary Disease (COPD) • A process characterized by the presence of chronic bronchitis, emphysema, or both, leading to the development of airway obstruction
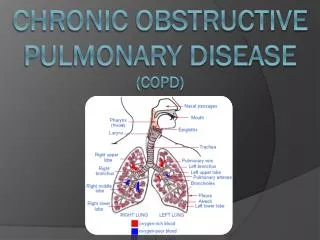
What is COPD? • COPD is a serious lung disease that makes it hard to breathe. • airways are partly blocked, which makes it hard to get air in and out • Emphysema- damage to air sacs in lungs • Chronic bronchitis- swelling of air passages that lead to lungs
Statistics • 3rd leading cause of death in the U.S. • Over 12 million are currently diagnosed and an estimated additional 12 million have it but haven’t been diagnosed
Etiology I am doing it, my etiology
COPD • Causes • Smoking (90%) • Environmental factors • Air pollution, confined kitchen areas • Genetics: α1-antitrypsin • Produced in liver • Protects lung against elastase • Elastase breaks down elastin • No elastin= no recoil • Deficiency liver and lung failure • Less than 1% of COPD patients • Without smoking
Emphysema • Imbalance of antiproteases & proteases Normal Cigarette smoke recruit neutrophils Cigarette smoke oxidation α1-antitrypsin deficiency Increased proteases
Emphysema • α1-antitrypsin deficiency & increased proteases • Collagen and elastin destruction • Flabby lung • ↓ recoil • Abnormal enlargement & destruction of alveoli • ↓ SA
Chronic Bronchitis • Cigarette smoke irritants inflammation of airway • Hyperplasia and hypertrophy of mucus glands • Hypertrophy of goblet cells increased mucus • Smaller airway + more mucus = mucus plug
Case Study • SB • Age 62 • Smoking history: 1 pack/day for 46 years • Quit 1 year ago
Physiology of Pulmonary System • Functions • Acid-Base Balance • Synthesize arachidonic acid • Prostaglandins, Leukotrienes • ACE converts Ang. I to Ang. II • Gas exchange • Surfactant • Immune defense
Basic Pathophysiology • Emphysema • Permanent enlargement of acini with alveolar destruction • Closure of small airways • Primary: Alpha-1 Antitrypsin deficiency (inherited) • Secondary: Inability to inhibit proteolytic enzymes (smoking, etc.) • Chronic Bronchitis • Hypersecretion of thick immobile mucus and productive cough • Mucus obstruction of bronchioles • Continuous bronchial inflammation * Common for patients to display both types
Emphysema • Pathophysiology • Smoke irritants cause inflammation of the epithelial • Protease activity increased by cytokines • Elastase, Cathepsin, Metalloprotease. • Imbalance of proteases and anti-proteases cause a breakdown on elastin in alveolar septa • Reduced elastic recoil and expiration • Eliminated portions of pulmonary capillary bed • Diminished airway caliber • Air-trapping (causing barrel chest) • Bronchoconstriction (caused by persistent inflammation)
Chronic Bronchitis • Pathophysiology • Smoking/irritants stimulate mucus production • Ciliary function impaired= reduced mucus clearance • Bacterial growth and inflammation= more mucus production • Bronchial/Bronchiolar walls thicken • Persistence involves bronchospasms and narrowing of the airways • Obstuction (Mucus + wall thickening + lumen narrowing) • Airway collapse in expiration
Effects on Energy • Affect on energy metabolism • Protein degradation - Cachexia
Acute Exacerbations • Accelerated loss of lung function and poor quality of life • Severe Pulmonary Hypertension • PA:A ratio >1 =pulmonary artery enlargement • Other effects: • Increase in dyspnea, hypercapnia, cough, and/or sputum production • New strains of bacteria or viruses; environmental factors • Ischemia, Heart Failure, Thromboembolism
Cor Pulmonale • Late stages • From chronic PAH: • Low PAO2 /Hypoxia causes pulmonary vasoconstriction • Can be reversed if PACO2 is cleared but… • Resistance to PA blood flow • Increased workload of RV • Peripheral edema noted
Emphysema • No mucus or cough • Barrel chest • ↓ lung plasticity & hyperinflation • Pressure around the lung greater • than pressure in the lung • Lung collapse • Trapped air • Expand anteroposteriorly
Emphysema • Breathing Habits • Lean forward • Stabilizes chest • Allows max expansion • Accessory muscles • Pursed lips • More air out before lung collapse
Emphysema • Older (>50) • Underweight, cachectic • Late cor pulmonale • Decreased DLCO • ↓ alveolar SA • “Pink puffers”
Chronic Bronchitis • Hypersecretion of mucus and chronic productive cough for 3 months for 2 consecutive years • Shorteness of breath, even at rest • Wheezing • Normal weight but often overweight
Chronic Bronchitis • V/Q Mismatch • V= Ventilation; air that reaches alveoli • Q=Perfusion; blood that reaches alveoli • Hypoxemia • Cyanosis around lips • “Blue bloaters” • Stimulates renal secretion of erythropoietin • High hematocrit • Vasoconstriction hypertension early cor pulmonale
Case Study “I am gasping for air” “I am coughing up a lot of phlegm” “I am always short of breath” No cyanosis or clubbing Wheezing Uses accessory muscles at rest
Spirometry • Pt inhales & then exhales as • much and as fast as possible • Measures • FVC • FEV1 • FEV1/FVC
Spirometry • Post-bronchodilator FEV1 / FVC <.7 confirms airflow limitation that is not fully reversible
Diffusion of Lung Capacity • DLCO • Patient inhales small amount of CO • Compare the amount exhaled by amount inhaled • Determines amount absorbed • ↓ indicative of emphysema but not chronic bronchitis
Prognosis • Not curable • Slow damage • Prevent exacerbation • acute change in symptoms to needing a change in therapy • dyspnoea • cough and/or sputum
Quality of Life • ADLs • http://www.youtube.com/watch?v=G3vmSDXHwMI
Case Study “I’m hardly able to do anything for myself…my husband had to help me out of the shower this morning.”
Treatment • No cure • Quite smoking • Walk to strengthen muscles needed for breathing • Avoid cold air • Avoid smoke, make sure no one smokes in your home • Reduce air pollution by getting rid of fireplace smoke and other irritants
Medications: Bronchodilators • Inhalers (Bronchodilators) work to relax the muscles around the airways, to help open them and make it easier to breathe. • Some Inhalers include: ipratropium (Atrovent), tiotropium (Spiriva), salmeterol (Serevent), formoterol (Foradil), or albuterol
Medications: Inhaled Steroids • Reduce lung inflammation • Most commonly used inhaled corticosteroids: fluticasone propionate, budesonide, and beclometasone dipropionate