Lung F unction T esting in School-Age Children
Lung F unction T esting in School-Age Children. Paul Aurora Great Ormond Street Hospital for Children, & Institute of Child Health, London. Structure of talk. Why bother? What do we need from a lung function test? What tests are available? Spirometry Other tests. Why bother?.

Lung F unction T esting in School-Age Children
E N D
Presentation Transcript
Lung Function Testingin School-Age Children Paul Aurora Great Ormond Street Hospital for Children, & Institute of Child Health, London
Structure of talk • Why bother? • What do we need from a lung function test? • What tests are available? • Spirometry • Other tests
Why bother? • LFTs aid diagnosis and prognosis, so are of benefit clinically and epidemiologically • Early identification of lung disease allows monitoring of progression • LFTs can be used as outcome measures to evaluate interventions
What is the test for? • For the researcher, lung function tests need to show differences between groups, at cross-section, and over time or with interventions • For the clinician, lung function tests need to discriminate between individuals, or to monitor change in an individual over time or with intervention
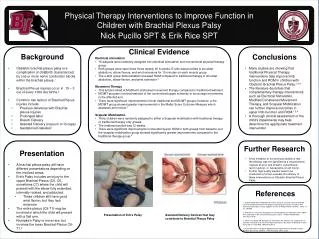
Airway function in infants with CF vs prospective healthy controls Average reduction of 22 % in FEV0.5 in infants with CF vs healthy infants after adjustment for body size, age, sex etc Ranganathan et al Lancet 2001 AJRCCM 2002 USA healthy London CF London healthy
So, what do we need to know first? • Precision – usually expressed as coefficient of variation • Variability/repeatability • Between subjects • Within subject, between occasions • Reference data • Standardisation
Between occasion repeatability Intervention Outcome 2 1 Time
Intervention Outcome 2 3 1 Time Between occasion repeatability Chan E, Thorax. 2003 Apr;58(4):344-7.
Accurate anthropometry essential for meaningful interpretation of results How often do you calibrate your stadiometer?
Quality control • Study by Arets et al (ERJ 2001) reported spirometry in 446 school-age children who were experienced in the test • Only 60% met ATS and ERS adult criteria for start of test • Only 15% met the criterion for forced expired time • Only 80% met the criteria for reproducibility • Conclusion – adult QC criteria are not appropriate for children
Commonly used techniques • Spirometry • tells you about airflow limitation and lung volumes • Plethysmography • tells you about airway resistance, total lung size, and trapped gas • Transfer factor • Tells you about alveolar function (also affected by pulmonary blood supply & VQ matching)
Less commonly used techniques • Gas washout tests • Tell you about gas mixing (small airway function, heterogenous changes in compliance) • Interrupter resistance (Rint) • Tells you about airway resistance • Oscillometry • possibly tells you about small airways
Diagnosingasthma • Change in lung function • After bronchodilator • After bronchoconstriction (exercise, dry air, methacholine) • Commonly use spirometry as outcome measure, but can use any airway test (eg airway resistance, gas washout)
Airway inflammation • Exhaled NO • Exhaled breath condensate • Induced sputum
Exercise tests • Maximal tests (eg bicycle ergometer) • Monitor VO2, VCO2, lactate production etc • Submaximal tests (6-min walk, 3-min step, shuttle) • Monitor walk distance, SpO2, HR, breathlessness scores
Other specialised tests • Fitness to fly (ask child to breath 15% O2, monitor SpO2) • Skin allergen testing (skin prick, skin patch)
What is a forced expiratory manoeuvre? • Breathe in to desired volume • exhale as fast as possible to RV • volume-time or flow-volume plots • easy for adults and children > 6, difficult for younger children, infants need assistance
What is measured from forced expiration? • Volume-time • Timed expired volumes, FEVt • MEF75-25 • Flow-Volume • PEF • Flow at fixed volumes, MEF%
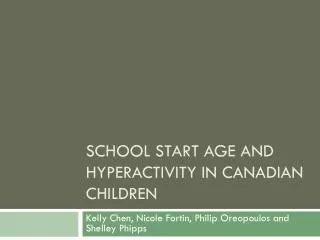
Forced Expiratory Flow-Volume Curve 12 PEF 9 MEF75% 6 Flow (L.s-1) MEF50% 3 MEF25% 0 100TLC 75 50 25 0RV Expired Vital Capacity (%)
What does the flow-volume curve tell you? • Flow-volume curves • maximal (MEFV) from TLC • partial (PEFV) from lower volume • slope of descending limb • inverse of time-constant of emptying • shape conveys information
Why measure forced expiration? • Expiratory flow-limitation is achieved with reasonable effort during forced expiration
Expiratory flow limitation • Once a certain minimum effort has been exceeded, maximum expiratory flow becomes independent of the effort applied • the maximum flow is thought to reflect the mechanical properties of the lungs and airways
Demonstrating flow-limitation: Isovolume pressure-flow curves • Series of forced expirations at different lung volumes • Driving pressure must be measured
Demonstrating flow-limitation 75% TLC 50% TLC 25% TLC
Demonstrating flow-limitation 75% TLC 50% TLC 25% TLC
Demonstrating flow-limitation • Isovolume pressure-flow curves • Increasing driving pressure • overlay curves • adding an oscillating pressure to jacket pressure during squeeze • applying negative pressure
NEP Equipment for assessing flow limitation during RVRTC Jones et al 2000
NEP to assess flow limitation - Jones et al AJRCCM 2000 Flow limitation achieved No Flow limitation
Theories to explain flow limitation • Equal pressure point (Mead et al. 1967) • Starling resistor (Pride et al. 1967) • Wave speed theory (Dawson et al. 1977)
Choose appropriate game • Set appropriate target • Allow sufficient trials
Body plethysmography • Airway resistance calculated from the relationship between pressure difference and flow • Total lung volume can be calculated by breathing against an occlusion
Multiple-breath washout • Tidal breathing test • The resident gas of the lung is ‘washed-out’ using air (eg SF6 or He washout), or oxygen (nitrogen washout) • The ventilation required to dilute the resident gas is a measure of (small) airway function
A = Wash-in phase B = Disconnection C = Washout
Interrupter technique: theory • Based on assumption that change in transpulmonary pressure observed immediately after sudden occlusion of airway is entirely explained by cessation of flow • Respiratory system resistance (Rrs) then calculated from change in pressure (Prs) and flow preceding occlusion • Assumes that pressure measured at mouth equilibrates along airways immediately after occlusion • Can now be measured by inexpensive portable device
Impulse oscillation / Forced oscillation: theory • The mechanical characteristics of a system may be calculated by relating the applied stress to the resultant deformation • During breathing, pressure is generated by the respiratory muscles to produce deformation of the lung • If transpulmonary pressure is varied in a frequency domain different from that of respiratory muscle activity, we can study mechanics related to the applied transpulmonary pressure
Impulse oscillation: technique • Signal of 6Hz or greater generated by computer, delivered through one or more loudspeakers placed at the mouth, at the chest or via a headbox (headbox aims to reduce upper airway artefact) • Measure angular velocity and frequency of applied pressure and resultant flow. From this can calculate the mechanical impedance of the respiratory system (Zrs, = Prs/ V’rs) • Pressure and flow are normally measured at same point (input impedance, Zrs,in)
Forced Oscillation Technique standard generator ‘head’ generator to minimize upper airway artefact
Nitric Oxide levels within the airway • NO formed in upper & lower respiratory tract • Diffusion into lumen conditions exhaled gas with NO • Alveolar NO is very low as NO taken up by haemoglobin in pulmonary capillaries • Nasal NO is high and may contaminate exhaled samples • Ambient NO may be very high. Measurement technique needs to prevent contamination of exhaled sample
Inhale (NO free air) • Exhale to RV • Inhale to TLC over 2-3s • No nose clip (unless subject cannot avoid nasal inspiration)Inspired air passes through a scrubber to eliminate ambient NO [recommend: FINO < 5 ppb]
Exhaled NO signal profiles • Flow 45-55 ml/sduration > 6s • NO profile:- washout phase- transition- plateau lasting >3s[NO] < 10% or if [NO] <5ppb, [NO] < 1ppb • Pressure 5-20 cmH2O. • Allow > 30s quiet breathing between tests • Repeatability: 2 tests with NO plateau within 10% of the mean