Download
1 / 22
220 likes | 410 Vues
Pulmonary adaptive responses against bacterial pathogens. J S Brown Reader in Respiratory Infection Centre for Respiratory Research Department of Medicine University College London. Adult community acquired pneumonia: CAP. incidence: overall 0.25%?

E N D
Pulmonary adaptive responses against bacterial pathogens J S Brown Reader in Respiratory Infection Centre for Respiratory Research Department of Medicine University College London
Adult community acquired pneumonia: CAP • incidence: overall 0.25%? • admissions 50/100,000 per year > 65 years • 50 - 80% mild - outpatient treatment • 50 - 20% admitted - 10 - 20% severe / ITU • - mortality 5 – 10% (20% UK audit) • - 65000 deaths per year in UK • who gets CAP? • - elderly: but only 50% cases >65 years • - smokers: attributable risk 51% • - comorbidities: attributable risk 14% • (lung /cirrhosis / renal disease / diabetesCNSdisease)
Causes of adult community acquired pneumonia [CAP] (Lim et al. Thorax 2001)UK hospitalised patients influenza 13% other viruses 4% Streptococcus pneumoniae Chlamydia pneumoniae 48% 13% Mycoplasma pneumoniae 3% Legionella 3% 20% 7% Haemophilus influenzae Unknown Staphylococcus aureus 1.5% Moraxella catarrhalis 2% 20% no pathogen identified Gram negative bacilli 1.4%
Causes of CAP worldwide (JSBrownRespirology 2009)
Streptococcus pneumoniae infections2nd commonest bacterial cause of death nasopharyngeal commensal 10% adults 50% infants Septicaemia 1 in 25 mortality 20% aspiration meningitis mortality 20% pneumonia 0 to 75 per 100,000 colonisations otitis media mortality 0%
Streptococcus pneumoniae infection epidemiology • suggests adaptive immunity to colonisation is important? • waning of adaptive immunity with age? Health Protection Agency, United Kingdom, 2008
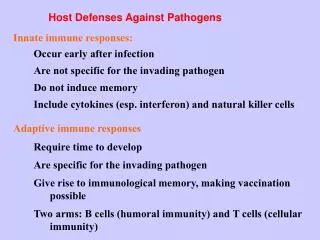
Immune response to S. pneumoniae pneumonia 3. Established pneumonia 2. Early lung infection 1. NP colonisation 4. Septicaemia • physical • defences • 2. mucosal • proteins • 3. lymphocytes • 4. phagocytes • physical • defences • 2. mucosal • proteins • 3.alveolar • macrophages 1. Complement 2. RE system 3. Circulating phagocytes 1. inflammatory exudate 2. phagocytes 3. CD4 and CD8 lymphocytes? Key immune effectors
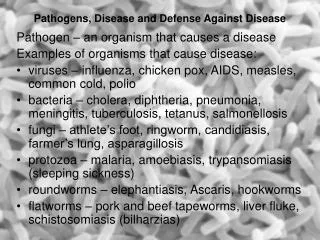
Mechanisms of adaptive immunity Hyper IgE syndrome IFN-gamma Th1 CD4 T-cell Mucosal repair IL-22 Th17 Antimicrobial peptides Antibody deficiencies Th2 IL-17 Antibody Chemokine release B-cell Phagocyte recruitment Phagocyte CD8 T-cell Cytotoxicity v. intracellular pathogens TAP syndrome?
Alveolar macrophages (AMs) • First-line phagocyte in lung • Large range of receptors for • - direct interactions with bacteria • - Indirect interactions • Airway lining fluid opsonins: • surfactant • complement • IgA and IgG Fc gamma Receptors Complement Receptors Scavenger Receptors Toll Like Receptors Mannose receptor / lectins
Bacterial phagocytosis by AMs can be saturated 1 hour + All bacteria killed 1 hour 1 hour +
EFFICIENT BACTERIAL CLEARANCE NO PNEUMONIA / BRONCHITIS • intact epithelium • efficient alveolar macrophages Do IgG and IgA improve S. pneumoniaeopsonisation in airways?? • low inoculum • low virulence strain BACTERIAL FACTORS HOST FACTORS
significant levels in IgG, IgA and IgM in airway lining fluid • IgG predominant x5 that of IgA • efficacy of IgG at promoting alveolar macrophage activity: • efficacy of IgA / IgM not clear…… Antibody and alveolar macrophages: IgG effect Gordon et al. Infect Immun 2000
Antibody and prevention pneumonia: • 1er and 2er IgG deficiency recurrent lung infections • therefore IgG essential for preventing lung infection • role of IgA unclear - IgA deficiency 1 in 400, only a subset develop recurrent lung infections • deficiency IgM also only sometimes associated with recurrent lung infection
Anti IgG, alveolar macrophages, and S. pneumoniae: mouse data Bacterial lung CFU inversely correlate with Ab level to Cps Ag • mice protected v pneumonia • after vaccination with: • protein antigens • conjugated capsule antigen • unconjugated capsule antigen • dead or live whole cells • but few data on mechanism(s) Jakobsen Infect Immun 1999
S. pneumoniae capsular polysaccharide vaccines and protection against CAP: • 23 valent unconjugated Pneumovax • - protects against septicaemia • - no evidence protects against pneumonia • conjugated vaccine • - 7 to 13 valent • - protects children against pneumonia (25%:) directly?? • - not used in adults yet • - major issue serotype with coverage: <30% CAP strains covered by Prevenar? IgG response too weak (unconjugated)? Host response poor due to comorbidity / age? Serotype coverage too restricted to detect effects? Wrong antigens?
Failure of clearance of initial S. pneumoniae infection neutrophilic consolidation
IL17 dependent immunity Invading S. pneumoniae increased mucosal: - chemokine release - antimicrobial peptides - mucosal repair Neutrophil recruitment IL-22 IL-17 Primed Th17 CD4 cells
Hyper IgE (Job’s) syndrome and pneumonia • triad of: raised IgE, abscesses, and pneumonia • infections with S. pneumoniae • mutations of STAT3, regulates cytokine responses • specifically causes a defect in CD4 Th17 response • demonstrates probable role for Th17 v. lung infection Milner Nature 2008
IL-17 dependent adaptive immunity and S. pneumoniae • required for immunity v. nasopharyngeal colonisation: • - after colonisation(Zhang J Clin Inv 2009) • - after vaccination with whole cell vaccine (Lu PLoS Pathogens) • mechanism: • neutrophil-dependent • increases neutrophil recruitment and efficacy • We don’t know whether protects against pneumonia…. • Antigen targets unknown…… (lipoprotein?)
Target antigens for natural adaptive responses to S. pneumoniae serotype dependent incidence in children with increasing age • capsule target for vaccine adaptive responses • may not be for natural responses: • wide range protein antigens • acquired immunity seems independent of capsule serotype • anti-protein response to colonisation often dominant • protein antigens maybe cross-protective Lipsitch, Plos Medicine, 2005
Summary and conclusions re. lung adaptive immunity v. S.pneumoniae • Antibody via improved alveolar macrophage and neutrophilphagocytosisv. important • Th-17 mechanisms also could be helpful • Natural adaptive immune responses can be directed against protein antigens • Need to aim for vaccination strategy that: • boosts S. pneumoniaeclearance from the lungs • therefore alveolar macrophage efficacy key • can protect against wide-range of strains • protein antigens need to be considered
Acknowledgments • UCL Centre for Respiratory Research • Dr Jonathan Cohen • Dr Suneeta Khandavilli • Dr Catherine Hyams • Dr Emilie Camberlein • Dr Jose Yuste • Dr Alejandro Ortiz Stern • Steve Bottoms • Erasmus Medical Centre, Rotterdam • Prof Alex van Belkum • Dr Corné de Vogel • UCL Biological Services Unit • UCL Institute of Child Health • Dr Helen Baxendale • Prof David Goldblatt • Prof Nigel Klein • Lindsey Ashton • UCL Dept Immunology • Dr Claudia Mauri • Dr Natalie Carter • Intercell AG, Vienna • Dr Carmen Giefing • Dr Eszter Nagy