Download
1 / 33
340 likes | 465 Vues
This clinical case study presents the journey of a 74-year-old woman diagnosed with irritable bowel syndrome 12 years prior, who ultimately underwent evaluation for suspected celiac disease. Despite treatment options that included Lomotil and Metamucil, her gastrointestinal symptoms persisted, resulting in significant weight loss and health deterioration. A series of diagnostic procedures led to a diagnosis of celiac disease. After adopting a strict gluten-free diet, the patient's condition improved dramatically, marking a significant turnaround in her health and quality of life.

E N D
Celiac sprue Un caso clinico dal web
Case Presentation January 1991 • J. N. is a 74 year old white female • Dx. 12 years ago with irritable bowel syndrome • Tx. with Tigan, Lomotil, Donnatal but worsened • Up to 8 loose, watery stools/day; abdominal pain; dec. energy; nausea; and 34 lb. wt. loss in 2 years • Work-up - Upper GI showed hiatal hernia • Pelvic U/S showed small cyst on left ovary
vertigo, iron deficiency anemia Meds: Inderal 20mg Meclizine 25mg wt. 99lb Rectal: no hemorrhoid or mass, +brown stool with mucous, heme - A: IBS P: Metamucil, high fiber diet, Lomotil Case Presentation
Case Presentation November 1991 (9 months later) • Post hysterectomy, 5-6 stools/day despite 8 tabs. Lomotil, Wt. 88 lbs., Abd. - benign, Stool - heme+ • Colonoscopy - Sessile polyp (benign adenoma) • Diverticular disease • EGD - Hiatal hernia and gastritis • Flat appearing duodenal mucosa (villous atrophy and chronic inflammation suggestive of celiac disease)
Case Presentation • Referred to dietitian for gluten-free diet education • Dec. 1991 - Strict diet, asymptomatic, Wt. 86 lbs. • Feels like a “reborn woman” • June 1992 - Strict diet, asymptomatic, Wt. 132 lbs. • June 1993 - Strict diet, asymptomatic, Wt. 141 lbs. • Aug. 1996 - Strict diet, asymptomatic, Wt. 142 lbs
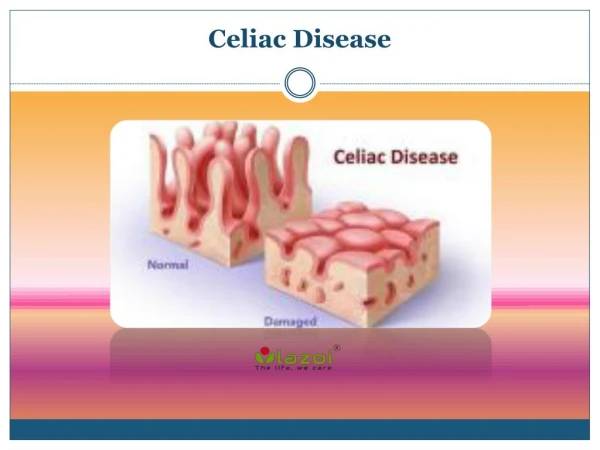
Introduction Key Elements • Evidence of malabsorption • Pathological damage to the small intestine • Response to a gluten-free diet
Etiology and Pathogenesis Environmental Factors • Cereal grains of wheat, rye, barley, and oats • Prolamins = alcohol-soluble proteins of gluten • 12 amino acid segment of the E1b protein of human adenovirus, serotype 12 • 89% of untreated celiac sprue patients • 17% of control subjects
Etiology and Pathogenesis Genetic Factors • 10% prevalence among first-degree relatives • 28-40% concordance rate between HLA identical siblings • 70-75% concordance rate between monozygotic twins • 90% have HLA-B8, HLA-DR3, or HLA-DQw2 haplotype • 25-30% of general population have these haplotypes • Only 0.1% of people with these haplotypes develop celiac sprue
Etiology and Pathogenesis Immunologic Factors • Humoral and cell-mediated mechanisms • Antigliadin antibody triggering the complement cascade • Anti-transglutaminase • Antigliadin antibody causing cytotoxic cell-mediated mucosal damage • Intraepithelial lymphocytes in the absorptive cells producing lymphokines
Pathology • Small intestinal mucosa affected (proximal>distal) • Length involved correlates with severity of disease • Villous atrophy and crypt hyperplasia decreasing the villous: crypt ratio • Columnar to cuboidal to squamous absorptive cell • Microvilli decrease • Abnormal tight junctions allow more permeability • Increased mitotic activity
Pathology • Increased numbers of intraepithelial lymphocytes, plasma cells, mast cells, and eosinophils • Continuum of changes (minimal to severe) • Injury occurs within hours of ingestion of gluten • Recovery takes weeks to months, but many never demonstrate improvement • Pathological changes are not pathognomonic
Clinical Features Gastrointestinal Symptoms • Women 20s - 30s, men - slightly later • Diarrhea, abd. distention, flatulence, weakness, lassitude, and weight loss most common • Stools are bulky, loose, pale, float, foul-smelling • Diarrhea usually in morning • Abd. distention and flatulence usually in evening • Abdominal pain is uncommon and may be the first sign of an underlying malignancy
Clinical Features Extraintestinal Symptoms • Anemia (iron, folate, and rarely B12 deficiency) • Poor absorption, sloughing cells, microerosions • Bleeding (vitamin K deficiency) • Osteopenia (bone pain and pathological fractures) • Decreased Ca++ and vitamin D absorption • Intraluminal binding of calcium • Tetany and secondary hyperparathyriodism
Clinical Features Extraintestinal Symptoms • Neurological deficits (hypokalemia and B12 def.) • Paresthesias, sensory deficits, ataxia, peripheral neuropathy • Night blindness (vitamin A deficiency) • Depression and anxiety • Menstrual irregularities and infertility
Physical Findings • Correlates with severity of intestinal involvement • Pallor • Wt. loss, wasting, loose skin folds, hypotension • Cheilosis, glossitis, aphthous ulcers • Doughy, protuberant, tympanic abdomen • Ascites and peripheral edema • Ecchymoses • Hyperkeratosis follicularis • Dec. DTRs or sensation, +Chvostek / Trousseau
Diagnostic Studies Malabsorption Studies • Previously the main diagnostic test • Very nonspecific • Unhelpful in asymptomatic patients • D-xylose test (decrease in serum or urine levels) • Sensitivity = 95% • Lactose intolerance test (inapprop. low glucose) • Breath hydrogen test (inapprop. high expired air hydrogen)
Diagnostic Studies Radiologic Studies • Upper GI barium study • Dilatation of small bowel loops • Coarsening and obliteration of mucosal folds • Nonspecific, thus little use in initial work-up • Irregularly narrowed segments c/w lymphoma • Rigidity c/w collagenous sprue • Osteopenia or pathological fractures on plain films
Diagnostic Studies Serologic Studies • Combination of tests may be adequate for screening high risk individuals • 2% incidence of IgA deficiency • Benefit from treating asymptomatic patients with positive antibody test and characteristic biopsy • Following levels helpful in assessing dietary compliance and disease progression/complications
Diagnostic Studies Histopathologic Studies • Endoscopic duodenal biopsy is the gold standard • Classical histology is not pathognomonic • Second biopsy demonstrating improvement on diet may be replaced by serologic markers • Biopsy (third) after gluten challenge not recommended unless patient is currently on gluten-free diet and initial biopsy not obtained • EGD may show flattening of duodenal folds
Associated Disorders Dermatitis Herpetiformis • 5% of celiac sprue patients have DH • Nearly 100% of DH patients have celiac sprue • Vesicles / excoriations which are pruritic / burning • Associated with HLA-B8 and HLA-Dw3 • Biopsy shows IgA deposits at dermal / epidermal junction • Treatment with gluten-free diet (slow) or dapsone (faster)
Associated Disorders Other Disorders • IgA deficiency - 10 times more frequent • Insulin dependent diabetes mellitus-4.1% have CS • Autoimmune thyroid disease - 4.8% have CS • Sjogren’s syndrome, SLE, vasculitis, RA • IgA mesangial nephropathy • Primary biliary cirrhosis, primary sclerosing cholangitis, inflammatory bowel disease
Treatment and Prognosis • Therapy of choice is lifelong gluten-free diet • Major lifestyle change as common foods have to be substituted / avoided compromising taste • Symptoms improve within days to weeks • Pathological changes take months or longer • Foods may be added back in small amounts (trial) • Most common cause of failed therapy is dietary noncompliance (dietary education is necessary)
Treatment and Prognosis • Those not responding to diet are termed refractory sprue - may respond to corticosteroids • Cyclosporine and azathioprine not proven • Many develop secondary lactase deficiency • Avoid milk products until stable • Replace vitamin and electrolyte deficiencies • Prognosis is excellent for those who respond to a gluten-free diet (majority)
Complications Malignancy • Twofold increase in developing malignancy - lymphoma (50%), carcinoma of esophagus, mouth, pharynx, larynx, and small intestine • Relative risk of lymphoma is 25-120x, greatest in men, older patients, and those untreated >10 years • Suspect when previous diet-responsive patient develops weight loss, abdominal pain, weakness malabsorption, pyrexia, lymphadenopathy
Complications Malignancy • Prognosis poor with surgical resection, XRT, and chemotherapy (9 month life expectancy) • Reason for increased incidence ? • Increased mitotic activity, increased mutations • Increased permeability to carcinogens • Damaged mucosa’s contact with oncoviruses • Strict gluten-free diet reduces risk to 1.2x normal
Complications • Ulcerative Jejunoileitis - 75% mortality • Ulceration and stricture formation - resection • Obstruction, perforation, bleeding, peritonitis • Collagenous Sprue • Subepithelial deposition of collagen • Tend to be refractory - corticosteroid trial • Neurological and Psychological • Sensory ataxia, numbness, tingling, pain, weakness, unsteady gait, depression
Summary • Sm. bowel malabsorptive disease (children/adults) • Intolerance to gluten (wheat, rye, barley, oats) • Abd. discomfort, diarrhea, wt. loss, extraintestinal • Sm. bowel bx (villous atrophy / crypt hyperplasia) • Response to a gluten-free diet (dec. complications) • Serologies aid in screening / following compliance • Prognosis is good as disorder is potentially curable • Potentially fatal disease if overlooked