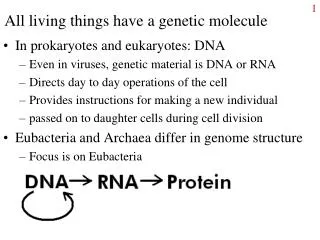
Living with dementia: making a difference through research
720 likes | 937 Vues
Living with dementia: making a difference through research. Professor Bob Woods Dementia Services Development Centre Wales Bangor University b.woods@bangor.ac.uk. Welcome back!. 2011 – What can we learn from people with dementia? 2012 – Dementia supportive communities

Living with dementia: making a difference through research
E N D
Presentation Transcript
Living with dementia: making a difference through research Professor Bob Woods Dementia Services Development Centre Wales Bangor University b.woods@bangor.ac.uk
Welcome back! • 2011 – What can we learn from people with dementia? • 2012 – Dementia supportive communities • 2013 – Making a difference through research
A quick recap:What is dementia? • An acquired impairment • Global cognitive functions (memory plus) • Self-care and day-to-day function • Clear consciousness • Usually progressive • Behavioural and psychological symptoms may include wandering, aggression, apathy, hallucinations, loss of inhibitions, repetition etc.
Types of dementia • Alzheimer’s disease - 40% • Vascular (multi-infarct) - 20% • Lewy Body dementia - 15% • Mixed Alzheimer’s & Vascular - 15% • Other (including alcohol-related, CJD, Pick’s etc) - 10% • Each type associated with distinct brain changes, evident at post-mortem
Prevalence of dementia in older people (UK Dementia Report, 2007)
Ageing population predicted to increase number of people with age-related conditions such as dementia • 37,000 people in Wales with dementia in 2007 • 50,000 people in Wales with dementia in 2021 • Number of people with dementia predicted to increase by 33% by the year 2021 • Gwynedd from 1,719 to 2325 • Anglesey from 905 to 1,223 • Conwy from 2,062 to 2,793
How old are people with dementia?(Prevalence figures for Conwy 2013 – UK Dementia Report)
National Dementia Vision for Wales 2011 – 6 commitments • To improve services • Younger people with dementia • Dementia Coordinators • Dementia targets • Timely diagnosis • General hospitals • Reduce inappropriate anti-psychotics • Support carers • Improve NHS in-patient units • To improve information • To raise awareness • To improve training • To support research • ‘Delivery Assurance Group’
Dementia research is the poor relation of medical and health research (Source: Alzheimer’s Research Trust, 2010) In the UK, for every person with cancer, £291 is spent on research; for dementia £61 is spent.
Prime Minister’s challenge on dementia (March 2012) • ‘As a society, we must make sure that people with dementia, their carers and families can be active citizens with the potential to live well with dementia at every stage of the condition.’ • ‘We would like people to feel confident that we are making significant progress towards prevention, treatment and cure in the UK, and to be able to say that they wanted to take part in research and were able to do so.’
Prime Minister’s challenge on dementia (March 2012) • ‘We will work towards recruiting 10% of patients into clinical trials. • Participation in high-quality research: • Consent to participate in research will be one of the conditions of accreditation for memory services.’
Research on dementia in Wales • Welsh Government fund NEURODEM Cymru – ‘Registered Research Group’ since 2006 – hosted by DSDC at Bangor • Cumulative project portfolio: 100 projects, with total value £41.6 million • Particular strengths: • Research on genetic factors (Julie Williams, Cardiff) • Research on Huntington’s disease (Anne Rosser, Cardiff) • Research on Parkinson’s disease (Huw Morris, Cardiff; John Hindle, Bangor) • Research on dementia care (Linda Clare, Bob Woods, Bangor) • Research on risk and prevention of dementia (Linda Clare, Bob Woods, Bangor; Ness Burholt, Swansea; Tony Bayer, Cardiff)
Opportunities to take part in high quality research • NEURODEM participant register: • agreement to be approached • Current projects include: • Effects of being bilingual on dementia • Individual cognitive stimulation (delivered by carer) • Maintaining function and well-being in later life • CFAS Wales (Anglesey & Dwyfor) • Lifestyle Matters • Agewell centres
Why take part in research? • Benefits to self: • Access to information or a potential new treatment approach, or contact with research team • Chance to do something you may find enjoyable • Ensure your perspective is represented • Benefits to others • Improve support / treatments available to people with dementia and their families in the future • Develop new knowledge that can help others
What have we learned in the last 12 months? • Reminiscence groups • Awareness in severe dementia • Cognitive stimulation • Life story books
Evaluating the effects of reminiscence groups for people with dementia and their carers: the REMCARE trial • Joint reminiscence v usual treatment • Pragmatic single-blind RCT • 8 centres in Wales & England • Up to 12 people with dementia and andand carers in each group • Treatment manual • 10 month period includes monthly maintenance sessions
Reminiscence groups for people with dementia and their care-givers: pragmatic 8-centre trial of: joint reminiscence and maintenance v. usual treatmentISRCTN42430123 • 'This project was funded by the National Institute for Health Research Health Technology Assessment (NIHR HTA) programme (project number 06/304/229) and will be published in full after peer review in Health Technology Assessment. Visit the HTA programme website for further project information.' • 'The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the HTA programme, NIHR, NHS or the Department of Health.'
Participants • 488 people with mild to moderate dementia (95% of target) • Mean age 77.5 • 71% of carers were spouses • 83% Alzheimer’s or mixed dementia (where recorded) • Community resident at outset
Participants - 2 • Recruited mainly from Memory Clinics and CMHTs • 268 randomly allocated to RYCT • 219 randomly allocated to ‘treatment as usual’ • 72% (350) available at ten-month follow-up (6% lost through death) • More attrition in control group (34% v 23%)
Primary outcome measures • Person with dementia – quality of life • QoL-AD (13 item self-report) • QoL-AD proxy (13 item carer-completed) • Care-giver – psychological distress • GHQ-28 • Results: no differences on these measures • Raised anxiety for family carers on sub-scale of GHQ-28 • Why no effect?
Attendance at RYCT sessions • 20% of those randomised to attend RYCT groups attend zero or one session • 29% attend less than half the planned 12 weekly sessions • 57% attended at least 3 of the monthly maintenance sessions • Compliance analyses • 3 months – attend 6 or more weekly sessions (70%) • 10 months – attend 3 or more monthly sessions (57%)
Results for those people who actually attend the groups • Improved autobiographical memory at 3 months • Improved quality of relationship (rated by person with dementia) at 10 months • Improved health related quality of life (EQ-5D) rated by person with dementia at 10 months • Increased stress for relatives at 10 months
Implications of joint approach • Carers will meet other carers • Carers will share knowledge of services (increased use of day services in treatment group) • Carers will share experiences • Carers will see other people with dementia • Carers may become more aware of other aspects of the dementia journey • Carers may see person ‘come alive’ in session and then return to ‘normal’ in between? • Could these aspects raise carers’ anxiety?
What do carers say? • A care-giver explaining why she would recommend the groups to a friend stated: • “people and carers in the same situations as oneself, they understand what we are going through” • Another commented on learning from other care-givers: • “(the group was) very good, it showed how other people dealt with their partner” • Another highlighted the effects on the person with dementia (the care-giver’s mother): • “At first I was sceptical about this work, thinking it would not do much, but I was amazed when, after and in between group sessions my mum was remembering the past and trying hard to remember more. It’s good for the participants to have 1:1 with a facilitator and feel important. I suppose the participant feels less worthy having no memory and not being able to do things, these sessions make them feel worthwhile and special again. They come away with more confidence I think.”
Next steps • The REMCARE final report is published as an HTA monograph • Further work is in progress analysing qualitative data collected alongside the trial • Further analyses will explore what is different (if anything) about those who continue to attend • Further analyses will examine mechanisms of change and identify predictors of who benefits • Comparisons with data from the SHIELD programme, where RYCT is being contrasted with a carer support programme, will further illuminate the REMCARE results • http://www.hta.ac.uk/project/1655.asp
What have we learned in the last 12 months - 1 • Reminiscence groups for people with dementia and their carers are generally enjoyed, but do not appear to have lasting effects on quality of life (the REMCARE study) • Some improvements for people with dementia who attend consistently • May contribute to increased carer anxiety • http://www.hta.ac.uk/project/1655.asp
Awareness in severe dementia? Often assumed that care home residents with severe dementia are lacking awareness of what is happening in their environment, especially where no longer able to express awareness through verbal communication. BUT still possible to identify signs of retained awareness by carefully observing the resident’s behavioural responses to his/her surroundings.
Awareness in severe dementia • Sensory appreciation still possible • Social stimuli most often elicit a response • We need to be more sensitive to the indications the person gives us of their response and interest • Eye movements • Facial expression • Sounds • Subtle movements
The AwareCare study(funded by MRC) • In 4 care homes in North Wales developed an observational tool that care staff could be trained to use • Uses a combination of natural and prompted triggers • Careful attention to response • Trial of staff training in use of the tool in 8 care homes in North Wales • Staff trained to observe carefully, and to use tool as a starting point for activity and communication • Results indicated improved quality of life (as rated by relatives) in homes where staff were trained to use the tool
‘Wendy’ • Wendy was not mobile, usually mute and sat with her eyes closed for most of the day. • However, when shown a picture, a very subtle flickering of the eyes to glance at the picture could be observed and sometimes she would respond with a whisper. • Furthermore, on one occasion when xxx began to play music to her and joked that it was a song that you could “boogie to”, Wendy responded with a strained, yet very deliberate smile and the staff were amazed that she still had such an ability.
What have we learned in the last 12 months - 2 • Quality of life (rated by relatives) of residents improved in care homes where staff were trained to use the Awarecare tool. • The tool helps staff recognise indicators of awareness in severe dementia
Cognitive stimulation (CST) groups • 14 Sessions (2 sessions / week) 45 minutes • 1) Physical games • 2) Sound effects, music • 3) Early memories • 4) Food • 5) Current affairs • 6) Faces / scenes • 7) Associated words • 8) Using objects • 9) Categorising objects • 10) Orientation (creation of map) • 11) Using money • 12) Number-related activity • 13) Word-related activity • 14) Quiz, consolidation
NICE-SCIE guidance on the management of the dementias (2006) www.nice.org.uk • People with mild/moderate dementia of all types should be given the opportunity to participate in a structured group cognitive stimulation programme … provided by workers with training and supervision … irrespective of any anti-dementia drug received …’
Maintenance Cognitive Stimulation trialOrrell, Aguirre et al. NIHR ‘SHIELD’ programme • ‘Making a difference – 2’ developed – 24 maintenance sessions • Open trial of ‘standard’ CST (7 weeks) • 236 participants randomised to continue once weekly sessions for 6 months (MCST) or treatment as usual • MMSE mean score 17.8 • Mean age 83 • 42% care home residents / 58% community resident (Day care etc.) • A third receiving ACHEIs (dementia drugs)
MCST preliminary results • After open trial, improved cognition and quality of life • At 6 month follow-up, MCST group have higher scores on QoL-AD • At 3 month follow-up, MCST group have higher scores on proxy QoL-AD and DEMQOL and ADL • Additional effect to that of ACHEIs
What have we learned in the last 12 months - 3 • Continuing Cognitive Stimulation groups weekly for 6 months after initial 7 weeks of sessions twice a week, leads to further improvements in quality of life • Adds to effects of dementia drugs
Identity and the person with dementia • Autobiographical memory • “It is an inescapable fact about human existence that we are made of our memories; we are what we remember ourselves to be” (Casey, 1989) • relates to sense of identity • reconstructive process - driven by emotions • possible disconnection from early memories
Reminiscence therapy – conceptual roots • Life review – Robert Butler (1963) • Erikson – integrity v despair • Person-centred care – the unique life story and biography of the person with dementia (cf. Kitwood) • Relationship-centred care – identity is maintained through interpersonal relating
Developing life story work • Previous study (Morgan & Woods, 2010) showed that life review leading to life story book led to improved autobiograhical memory and reduced depression in care home residents with dementia – books highly valued • How important is the process of life review as opposed to the tangible life story book? • Life review based life story books compared with ‘gift’ life story books produced by relatives • PonnuSubramaniam - PhD project
Life Story Books The idea of life story books or ‘This Is Your Life’ type scrapbooks has been adapted from child care work (Gibson, 1994). The story book, itself, is created by the person, using the person’s choice of pictures, props and words. The life story book is a pictorial reminder of an individual’s life as directed by the individual. The book include the items the individual chooses as important to him /herself. The caregiver can contribute by providing pictures and memorabilia from which the individual can select
Examples from James’s Life Story Book Childhood “My childhood life was very hard...difficult.... Once at age of 14, I ran away from my home and tried to join navy...they found out about my age...I was too young to join navy at that time...the navy people send me back home...my father got mad with me” – James laughing recalling his memory; 2nd Feb 2011
Examples from James’s Life Story Book (cont...) “My wife and I loved our Malta holiday. Out of all our holidays...Malta holiday was the best...we really enjoyed...except the mosquito bites... (laughing)! - James Mary and James – Malta Holiday
Examples from John’s Life Story Book PHOTOGRAPHS REMOVED This is John’s wife Emma. The photo was taken before they got married. They used to cycle (push bike) together. John used to cycle 20 miles from _________ to ___________ to meet Emma on the weekends. He stayed at his mother-in-law’s house at No. _____________. From John’s LSB: Page 8
Examples from John’s Life Story Book (cont...) PHOTOGRAPHS REMOVED John with his brand new motorbike. He was famous among his friends as ‘JOHN MOTORBIKE’. Only John had a motorbike among his friends. He is a Big Gun! After this motorbike he bought his first car. This little car had 3 wheels and was red in colour. - From John’s LSB: Page 10
Examples from Sarah’s Life Story Book ___ Carnival was a major part of Sarah’s life. She actively took part in many events and activities in ____ Carnival throughout her life. Above: Sarah was crowned as ____ Queen in ___ Carnival in the year of 1933. She was 11 years old. -From Sarah’s LSB: Page 7
Examples from Sarah’s Life Story Book (cont...) PHOTOGRAPHS REMOVED 52 years later, Sarah was crowning Queen Carol, ___ Carnival queen in 1985. Sarah was 63 years old. -From Sarah’s LSB: Page 38