Topic: Ankle Injuries
Topic: Ankle Injuries. Content:. Functional Anatomy; Acute Ankle Injuries; Ankle Examination; Lateral Ligament Injuries (Ankle Sprain); Medial Ligament Injuries; Pott's Fracture; Persistent Ankle pain; Some X-ray of Ankle Injuries;. ACUTE ANKLE INJURIES. Functional anatomy:.

Topic: Ankle Injuries
E N D
Presentation Transcript
Topic: Ankle Injuries
Content: • Functional Anatomy; • Acute Ankle Injuries; • Ankle Examination; • Lateral Ligament Injuries (Ankle Sprain); • Medial Ligament Injuries; • Pott's Fracture; • Persistent Ankle pain; • Some X-ray of Ankle Injuries;
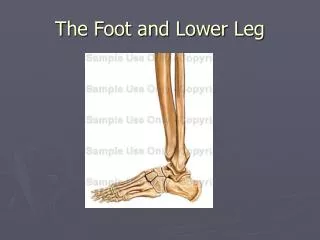
ACUTE ANKLE INJURIES Functional anatomy: The ankle contains three joints: 1. Talocrural (ankle) joint; 2. Inferior tibiofibular joint; 3. Subtalar joint; • The talocrural or ankle joint is a hinge joint formed between the inferior surface of the tibia and the superior surface of the talus. • The inferior tibiofibular joint is the articulation of the distal parts of the fibula and tibia.
The subtalar joint, between the talus and Calcaneus, is divided into an anterior and posterior articulation separated by the sinus tarsi.
Ligaments of the Ankle: Lateral malleolus calcaneofibular ligament long plantar ligament ligameni Lateral View
Long plantar ligament Calcaneonavicular ligament Medial view
Acute Ankle Injuries: • Ligament sprain (Lateral ligaments ) (Most Common); • Ligament sprain • Medial ligament • AITFL • Peroneal dislocation • Fractures • Laterai/medial/posterior Malleolus (Pott's) • Talar dome • Tibial plafond • Base of the fifth metatarsal • Anterior process of the calcaneus • Lateral process of the talus • Posterior process of the talus • Dislocated ankle • Tendon rupture
Examination: Examination of the ankle requires assessment of the degree of instability present and the grading of the ligamentous injury. Examination should detect functional disability such as loss of range of motion, reduced strength and reduced proprioception, etc 1. Observation (a) standing (b) supine 2. Active movements (a) plantarflexion/dorsrflexion (b) inversion/aversion 3. Passive movements (a) plantarfiexion/dorsiflexion (b) inversion/eversion 4. Resisted movements 5. Functional tests (a) lunge test (b) hopping 6. Palpation (a) distal fibula (b) lateral malleolus (c) lateral ligaments (d) talus (e) peroneal tendon (t) base of fifth metatarsal (g) anterior joint line (h) dome of talus (i) medial ligament (j) sinus tarsi
Special tests (a) Anterior drawer (b) Lateral talar tilt (c) Proprioception
Lateral Ligament Injuries: Ligamentous injuries around the ankle joint are among the most common sporting injuries, especially in jumping sports (e.g. basketball, volleyball). Lateral ligament injuries occur in activities involving rapid changes in direction, especially on uneven surfaces. They are also seen when contact with another competitor's feet causes imbalance in jumping or landing.
FIGURE 1. Grading of sprains. (A) The grade I sprain is characterized by stretching of the anterior talofibular and calcaneofibular ligaments. (B) In the grade II sprain, the anterior talofibular ligament tears partially, and the calcaneofibular igament stretches. (C) The grade III sprain is characterized by rupture of the anterior talofibular and calcaneofibular ligaments, with partial tearing of the posterior talofibular and tibiofibular ligaments.
Treatment: Initial Management: The initial management of lateral ligament injuries requires the RICE regimen. This is probably (the single-most important factor in treatment, particularly with grade I and grade II injuries). As well as hot showers, heat rubs. Reduction of Pain and swelling: Pain and swelling can be reduced with the use of electrotherapeutic modalities (e.g. TENS, interferential stimulation, magnetic field therapy). Analgesics may be required. Gentle soft tissue therapy and mobilization after the first 48 hours also may help to reduce pain. Restoring of Full Range of Motion: The patient may be non-weight-bearing on crutches for the first 24 hours but should then commence partial weight-bearing in normal heel-toe gait. It will be necessary from this stage to protect the damaged joint with strapping or bracing. As soon as pain allows, active range of motion exercises can be commenced.
Muscle Conditioning: Strengthening exercises should be commenced as soon as pain allows. Active exercises should be performed initially with gradually increasing resistance Exercises should include plantarflexion and dorsiflexion, inversion and eversion. Eversion strength is particularly important in the prevention of future lateral ligament injuries. Weight-bearing exercises should be commenced as soon as possible. Restoration of Proprioception: Proprioceptive retraining exercises can be commenced early in the rehabilitation program and should be gradually progressed from balancing on one leg to the use of the rocker board and ultimately to functional activities while balancing. Functional Exercise: Functional exercises (e.g. jumping, hopping, twisting, figure-of-eight running) should be commenced when the athlete is pain-free, has full range of motion and adequate muscle strength and proprioception.
Functional activity while Balancing Rocker board
Return to Sports: Return to sport is permitted when functional exercises can be performed without pain during or after activity. While performing rehabilitation activities and upon return to sport, added ankle protection is required. This can be provided either with taping or bracing. Treatment of grade III injuries: Treatment of grade III ankle injuries requires initial conservative management over a six-week period. If the patient continues to make good progress and is able to perform sporting activities with the aid of taping or bracing and without persistent problems during or following activity, surgery may not be required. If, however, despite appropriate rehabilitation and protection, the patient complains of recurrent episodes of instability or persistent pain, then surgical reconstruction of the lateral ligament. Following surgery, it is extremely important to undertake a comprehensive rehabilitation program to restore full joint range of motion, strength and proprioception.
Medial ligament injuries: Medial ligament injuries do not occur as frequently as lateral ligament injuries because the deltoid ligament requires considerable force to be damaged. Occasionally they may be seen in conjunction with a lateral ligament injury. Medial ligament injuries may occur with fracture of the medial malleolus or damage to articular surfaces. Treatment: Medial ligament sprains should be treated in the same manner as lateral ligament sprains, although return to activity may be prolonged. Pott's fracture: A fracture affecting one or more of the malleoli (lateral, medial, posterior) is known as a Pott's fracture. It can be difficult to distinguish clinically between a fracture and a moderate to severe ligament sprain. Both conditions may result from inversion injuries, with severe pain and swelling.
Persistent ankle pain: In most cases of ligament sprain, the patient progresses satisfactorily through the rehabilitation process. However, there is a significant group of patients who do not progress well and complain of persistent pain. It may be due to the following conditions: • inadequate rehabilitation • osteochondral fracture of the dome of the talus • dislocation of the peroneal tendons • chronic synovitis of the ankle joint • chronic ligamentous instability • sinus tarsi syndrome • anterior impingement syndrome • posterior impingement syndrome • anterolaleral impingement • rupture of the tibialis posterior tendon • reflex sympathetic dystrophy (RSD)
Other fractures: • avulsion fracture of the base of the fifth metatarsal • fracture of the lateral process of the talus • fracture of the anterior process of the calcaneus • fracture of the posterior process of the talus An ankle ligament injury that is inadequately rehabilitated may present with persistent pain and loss of function. This usually occurs with increased activity levels. The common problems associated with inadequate rehabilitation are a loss of range of motion in the ankle joint (especially dorsiflexion),weakness of the peroneal muscles and impaired proprioception. Management involves restoration of full dorsiflexion by active and passive mobilization of the ankle joint, a program of strengthening exercises for the peroneal muscles and proprioccptive exercises.
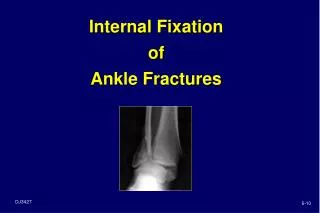
Distal Fibula fracture with associated medial deltoid ligament disruption. This injury is frequently the result of the foot being planted with a valgus load applied to the leg.
Ankle dislocation with no fractures. This takes a high degree of trauma and force. In this case this was generated as the result of a high flip off of a trampoline and impact with the ground. The ankle was in a plantar flexion and inverted position upon impact. This was an open dislocation.
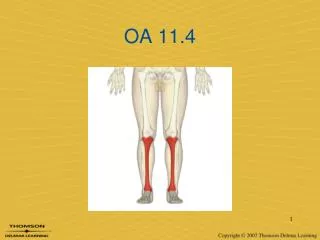
These X-Rays show a fracture of the proximal end of the 5th Metatarsal. This fracture is commonly called a "Jones Fracture".