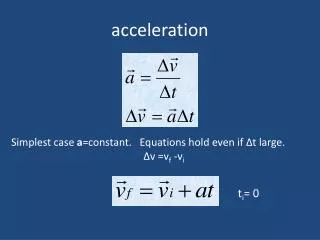
ACCELERATION
ACCELERATION. © Col (Dr) Pierre Erasmus. ACCELERATION. Introduction Aircrew can be insulated from most environmental stresses of flight such as heat, hypoxia and noise. However this is not true for acceleration. As a/c become more agile the worse there acceleration stresses.

ACCELERATION
E N D
Presentation Transcript
ACCELERATION © Col (Dr) Pierre Erasmus
ACCELERATION • Introduction • Aircrew can be insulated from most environmental stresses of flight such as heat, hypoxia and noise. • However this is not true for acceleration. • As a/c become more agile the worse there acceleration stresses. • There is unfortunately no anti-gravity device. • G-suits are not anti-gravity devices but just alleviates the effects. • With new aircraft operating in excess of 8G the human is operating at the limit of his performance. • Of particular concern is the potential of for G-induced loss of consciousness or G-LOC
ACCELERATION • Forces due to acceleration are vector quantities having proportion both of magnitude and direction. • Acceleration occur whenever there is a change in velocity, direction of motion at uniform velocity. • Forward acceleration causes a backwards acting inertial force. • Centripetal force will be sensed as the resultant centrifugal force. The effect on the body will depend markedly upon its orientation relative to the force vector.
ACCELERATION • EFFECT OF ACCELERATION DEPENDS ON: • Magnitude: Measured in units of G, this being the ratio of the applied force to the standard acceleration of gravity g, or 9,81m/s². Thus, 5G is equal to an acceleration of 49,05m/s² and the weight of the body is increased fivefold. • Direction: The vector direction of acceleration forces is defined according to a three-coordinate system based upon the long axis of the body. • Duration: Classified into: • a. Impact acceleration acting for a second or less. • b. Sustained acceleration acting for a second or more.
ACCELERATION • NOMENCLATURE FOR VECTORS OF ACCELERATION AND INERTIAL FORCE • DirectionDescriptionStandardVernacular • Upward s Positive G +GZ Eyeballs down • Downwards Negative G -GZ Eyeballs up • Forwards Transverse +GX Eyeballs in • supine G • Backwards Transverse -GX Eyeballs out • prone G • To right Left lateral G +GY Eyeballs left • To left Right lateral G -GY Eyeballs right
Supine G • Restraint: In a crash the occupant will continue along his initial velocity vector unless acted upon by a force. This can be done in a controlled manner through the use of a restraint harness or uncontrolled by him striking surrounding structures. • Site of action: Sustained acceleration affects all parts of the body but in the dynamic situation of impact differential forces occur. • Rate of onset: If the onset time of an impact force is comparable to the natural undamped frequency of the injury mechanism then the system will be excited and overshoot can occur.
ACCELERATION • Physiology of sustained +GZ acceleration • Effects similar to those of moving from the lying to standing posture. • Primary effect is on the cardiovascular system in the form of increase in hydrostatic pressure gradients. • 1 GZ BP at brain level is 22 mmHg lower than at heart level. At 5 GZ BP at brain level will fall to 10 mmHg. This effect is immediate and inevitable. • The heart and diaphragm fall and the heart to brain distance increases.
ACCELERATION • Hydrostatic increase in intravascular pressure below heart level causes vascular engorgement, especially the veins in legs and abdomen, which causes a decrease in the circulating blood volume and decreased venous return. • Raised intravascular and transmural pressure causes extravasation of fluid into the tissues with a further slow but progressive loss in circulating volume. • The initial fall in BP causes stimulation of the carotid baroreceptors and an increase in heart rate and peripheral resistance with a little restoration of BP at head level.
ACCELERATION • Local circulatory demands acts in opposition to the generalised vasoconstrictor response with a redistribution of the available cardiac output with the myocardium and brain receiving disproportionately more blood flow. • Owing to the intraocular tension which must be overcome to permit retinal perfusion, the blood supply to the eye fails at about 1GZ lower acceleration than that to the brain. • Gradual onset will lead to greyout with tunneling up to blackout and finally G-LOC. With rapid onset retinal Oxygen allows vision to be maintained for 4-5 seconds. • G-LOC is frequently followed by fitting, with flailing of the arms and a period of relative incapacitation.
ACCELERATION • The gradient of transpulmonary pressure stems from the weight of the lung tissue so that at +5GZ the gradient increases fivefold to about 1cm water per cm vertical distance. Thus for a lung 30cm tall there will be 30cm water difference in transpulmonary pressure from apex to base with gross changes in regional alveolar pressure and regional alveolar ventilation with the following: • The terminal airways close off with ventilation of the overperfused area ceasing. • Absorption of the trapped gas is delayed by the presence of Nitrogen but when 100% Oxygen has been breathed the entire gas volume will be rapidly absorbed and the lung collapses, called acceleration atelectasis.
ACCELERATION • If maintained, +GZ leads to vasovagal syncope. This is caused by the continued loss of circulatory blood volume with eventual breakdown of the cardiovascular compensatory mechanism causing a bradycardia, fall in peripheral vascular resistance and hypotension with loss of consciousness.
ACCELERATION • Tolerance to +GZ acceleration • Anti-G suit: Counter pressure acts on capacity vessels to decrease their transmural pressure and so reduce the pooling of blood and extravasation of fluid. • Anti-G straining manoeuvre: Combination of generalised muscle tensing, straining,and a forced expiratory effort. • Positive pressure breathing: The application of positive pressure through the aircraft breathing regulator. Reduces muscle fatigue.
ACCELERATION • Physical conditioning: Modest weight training of all muscle groups increases the time for which high-G can be tolerated. • Centrifuge training: An effective way of teaching an efficient AGSM and so raise G-tolerance. • Posture: Crouching forward and raising the rudder pedals assist G-tolerance by reducing the vertical heart-brain distance and improving venous return from the legs.
ACCELERATION • G-LOC
ACCELERATION Risk factors • Intercurrent illness. • Heat Stress. • Lay off. • Inadequate diet. • Fatigue. • Lack of sleep. • Excessive alcohol. • Hyperventilation.