Download
1 / 27
300 likes | 610 Vues
In the Clinic - Gout. Team Meeting Presentations. Risk Factors for Gout. Hyperuricemia Male sex if <60 Obesity High purine diet (red meat; shellfish) Alcohol (esp beer and spirits) and high fructose drinks Medications (thiazides; cyclosporine) CKD Lead exposure Organ transplantation

E N D
In the Clinic -Gout Team Meeting Presentations
Risk Factors for Gout • Hyperuricemia • Male sex if <60 • Obesity • High purine diet (red meat; shellfish) • Alcohol (esp beer and spirits) and high fructose drinks • Medications (thiazides; cyclosporine) • CKD • Lead exposure • Organ transplantation • Specific diseases (htn, DM, hyperlipidemia, hematologic malignancies; genetics
Are there effective strategies for primary prevention of gout? • Dietary modifications, weight loss • Pharmacologic therapy is not recommended when hyperuricemia is assymptomatic • Pharmocologic therapy is recommended in pts on chemo for hematologic malignancies • Uric acid lowering drugs and hydration prevent secondary gout due to tumor lysis • Without this treatment, uric acid nephropathy with tubular obstruction can develop
Is gout associated with increased risk for CV disease and can this be prevented? • Both CV disease and gout are associated with serum markers of inflammation • CV disease risk is increased in persons with gout or hyperuricemia • Opinions differ on whether the association of an elevated serum urate level with increased CV disease is modifiable
What symptoms and physical findings suggest gout? • Warmth, swelling, redness and severe joint pain • Of first attacks, 90% are monoarticular • Common sites of crystal deposition, tophus development: helix of the ear, lower extremities • Other sites: periarticular structures (bursae, tendons) • Crystals are more likely in previously diseased joints • Other forms of arthritis increase gout risk
Symptoms and Findings • Episodic self-limited joint pain, swelling, erythema • Attacks often occur at night or in early morning • Trauma may trigger release of crystals into joint space • Attacks often subside in 3-14 days without treatment
Tests to Diagnose Gout • Serum urate level- may be normal in acute flare • CBC with differential • Synovial fluid or tophus aspirate examination • Polarizing scope, cell count culture • Radiography – to r/o other causes or for findings suggestive of chronic gout
Value of radiography in the diagnosis of gout • Early in course- to r/o other conditions • Later in course – can show prominent, proliferative bony reaction • Gout related tophi cause bone destruction away from the joint • Gout less likely to cause joint space narrowing than psoriatic arthritis or rheumatoid arthritis
Differential Diagnosis of Gout • Rheumatoid arthritis • Symmetrical polyarthritis in small joints of hands and feet • Hand involvement more likely than in gout • Subcutaneous nodules in 20% • XRAY – soft tissue swelling; diffuse joint space narrowing, marginal erosions of small joints, osteopenia
Differential Diagnosis of Gout • Pseudogout – calcium pyrophosphate deposition disease • Appears in unusual places - elbows, wrists – without trauma • Affects 10-15% >65 • XRAY – looks like RA or osteoarthritis but with bony repair • Cartilage calcification • Triangular cartilage - pathognomonic
Differential Dx of Gout – cont’d • Septic Arthritis – • Fever, arthritis, great tenderness • Up to ½ have concomitant RA • Source is often evident • Diagnose and treat immediately to avoid joint destruction
Differential Diagnosis Gout- Cont’d • Cellulitis – gout often mistaken for cellulitis also • Erythema, swelling of the extremity, very tender, febrile • Often previous surgery or infection at the site • Xray – soft tissue swelling • Staph/strep most likely
Differential Dx- Gout – Cont’d Osteoarthritis – bony enlargement without signif inflammation – usually – May often involve the halus valgus – as in gout Psoriatic arthritis – DIP’s often, nail changes – XRAY central erosions, subchondral sclerosis, bony repair signs;uric acid levels might be high due to proliferative skin changes Sarcoidosis – acute disease can involve ankles – look for subcut nodules, erythema nodosum Assoc parotits, uveitis, hilar adenopathy, lung involvement
When to consider hospitalizing a patient with gout? • To distinguish gout from septic arthritis • Joint fluid analysis • Empiric antibiotics until diagnosis is clear • Repeated synovial fluid analysis if needed for culture, urate crystals, cell counts • To control pain Aspiration of joint fluid may help Gout is one of the most painful conditions
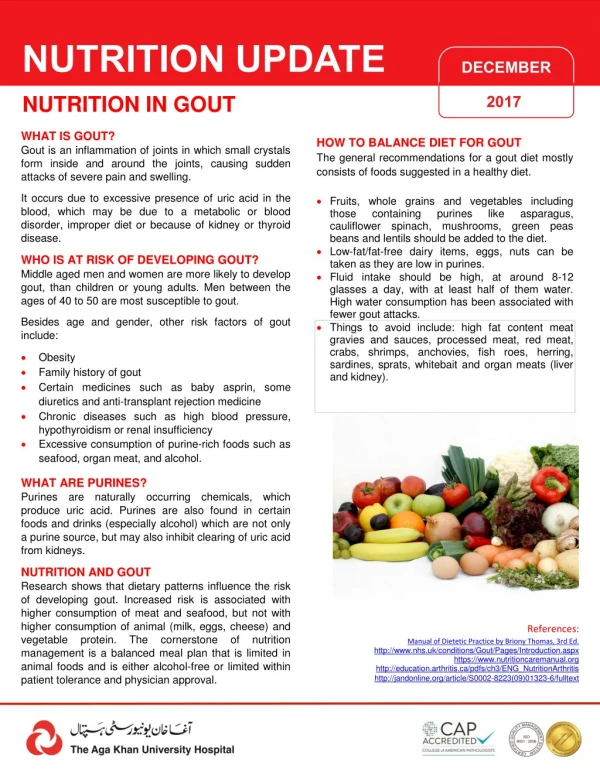
Non Drug Therapy in Gout • Reduce high purine foods in diet • Reduce alcohol and high fructose drinks • Weight loss – to decrease urate levels • Hydration • Diet high in fiber, vitamin C, folate • Replace medications that reduce uric acid excretion whenever possible
Diet Issues • High purine animal and fish sources • Red meat, meat extracts, organ meats, seafood • Yeast products – baked goods and beer • Mushrooms, spinach, asparagus, cauliflower • Legumes – peas, dried beans
Drugs for Acute Gout • NSAIDS • First line –analgesic/antiinflammatory • Ibuprofen and Naproxen better tolerated than indomethacin; don’t use aspirin • Start at higher dose and taper over 1 week • Side effects as usual • Caution in elderly • Don’t use in anticoagulated patients • Colchicine (oral) • Most effective if started 12-36 hours after onset • Lower doses reduce side effects (0.6 mg tid) • Side effects – GI, bone marrow suppression, myopathy, neuropathy, dermatitis, urticaria, alopecia, purpura • Myelosuppression can be severe at high doses; reduced with a short course • Caution when using other CYP3A4 inhibitors • Reduce dose for renla or hepatic dysfunction; avoid if on dialysis • Caution in elderly
Drugs for Acute Gout • Corticosteroids (oral) • For polyarticular gout when NSAIDS contraindicated • Side effects • Corticosteroids (intraartiular injection) • For monoarticular gout when NSAIDS not ideal • Side effects – risk for damage to nerves, tendons, vascular structures; joint infection risk; usual oral steroid risks • Rule out infectious cause before injecting join • Opiates – • For severe pain • Oral combinations of oxycodone, hydrocodone, codeine • Severe cases – morphine IV or SC • Short term - until inflammation resolved
Drugs to Prevent Gout and Complications of Hyperuricemia • To prevent growth of crystalliine deposits • Deposits can lead to chronically stiff, swollen joints and debilitating arthritis • To reduce tophi • To prevent flare recurrence • 60% flare again in 1 year, 78% within 2 • Subsequent attacks may last longer, involve more joints • To prevent uric acid stones • Occurs in 10-40% of persons with gout • Goal is to reduce urate <6 mg/dl
Drugs to prevent gout and complications of hyperuricemia • Allopurinol • Start 100-200 mg/d, increase by 100 mg.d every 1-4 weeks; reduced dose for CKD • Not in acute attack, concurrent colchicine may reduce risk for flare • Watch for hypersensitivity syndrome • Other side effects – rash, fever, headache, uritcaria, interstitial nephritis • LFTs and CBC monitored • Febuxostat • Start 40-80 mg/d; increase to achieve goal urate level • Steady state urate after 2 week use • LFT abn, diarrhea, headache, nausea, rash • No dose adjustment needed in mild to mod CKD
Other Drugs to reduce Uric acid level • Rasburicase • To prevent tumor lysis • Not if G6PD deficient • Start 24 hours before chemo • Probenicid • 0.5-2 mg /day divided 2X/day, dose adjust until urate level normalizes • Uricosuric – use only if underexreter • Don’t use with aspirin • Increases methotrexate toxicity • Rare anaphylaxis • Not effective in pts with signif CKD
Drugs to prevent Gouty attacks • Colchicine (oral) • Dose and use depends on cr clearance; avoid if <10 ml/min • Continue for 6 months after serum urate <6 or until tophi disappear • Use caution with other CYP3A4 inhibitors • May need to dose reduce with calcium channel blockers • Side effects GI intolerance, bone marrow suppression, dermatitis, urticaria, alopecia, purpura • Myopathy, neuropathy may increase with renal disease or with statin use • Avoid in severe liver disease
Indications for long term drug therapy to prevent gout and complications of hyperuricemia • At least 2-3 acute attacks of gout • Tophaceous gout • Severe attacks or polyarticular attacks • Radiographic evidence of joint damage from gout • Nephrolithiasis • Identifiable inborn metabolic deficiency causing hyperuricemia
When to think about referring for specialty consultation… • Consult with a rheumatologist or orthopedist • When joint sepsis is suspected • When gout is poorly controlled • When diagnosis is unclear • When gout occurs with other forms of arthritis • To aid in deciding on timing of initiation of meds or complicated regimens • Consult with rheum in pts with inherited metabolic disease for patients aged <20 with gout • Consult with nephrologist for help managing pts with CKD and/or urate nephropathy