Download
1 / 31
310 likes | 320 Vues
Explore the progress in quality and safety initiatives at Hadassah through completed projects and publications. Highlights include coronary revascularization, surgery quality, and infection reduction.

E N D
Quality & Safety at Hadassah A Progress Report September 12, 2006 Mayer Brezis, MD MPH, Professor of Medicine Center of Clinical Quality & SafetyChairman, Quality & Safety Committee
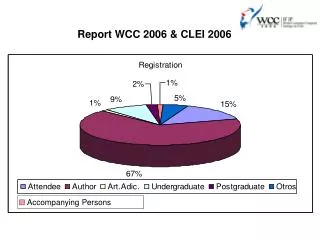
Quality at Hadassah: some statistics 36 projects completed as MD or MPH theses; 20 peer-reviewed publications
Outline of presentation • Appropriateness of Coronary Revascularization • Quality of Elective Surgery for Inguinal Hernia Repair • Reduction of Neurosurgical Shunt Infections • Quality of Reconstruction Surgery After Mastectomy • Hand-washing by Medical Staff • Progress on Previous Projects • Evaluation of Specific Patient Care
Appropriateness of Coronary Revascularization Procedures at Hadassah Hospital: Adherence to Clinical Practice Guidelines Dr. Dalit Cayam-Rand, Dr. Ronny Alcalai, Prof. Amir Elami & Prof. Mayer Brezis Heart Institute, Department of Cardiothoracic Surgery & Center for Quality & Safety, Hadassah Coronary Artery Bypass Graft (CABG) surgery Percutaneous Coronary Intervention
Development of guidelines • Institutional guidelines were developed by senior cardiologists and cardiac surgeons at Hadassah, in collaboration with the Center for Clinical Quality & Safety. The guidelines were derived from those of the American College of Cardiology and Heart Association, adapted on basis of most recent literature. • The guidelines were approved by staffs of both the Heart Institute and Department of Cardiothoracic Surgery at Hadassah. • Six months after approval, implementation of guidelines was examined.
Sample from guidelines CABG is the first option for: 1. Left main coronary artery stenosis (level of evidence A) 2. Obstruction of origin of left anterior descending (LAD) artery and of circumflex artery (level of evidence A) 3. Triple vessel disease, with diabetes or renal failure (level of evidence A) 4. Proximal LAD with high risk for angiographic treatment (level of evidence B) 5. Triple vessel or proximal LAD and failure of angiographic treatment (level of evidence C)
Rate of adherence to guidelines Overall rate of inappropriateness: 6%Corrected rate (out of referrals): 8%
“For patients with two or more diseased coronary arteries, CABG is associated with higher adjusted rates of long-term survival than stenting.” Hannan, E. et al. N Engl J Med 2005 352: 2174-2183
“CABG is still the best treatment for multivessel and left main disease” Professor David P TaggartCardiovascular Surgery, Oxford BMJ, April 2, 2005
Conclusion • Overall adherence to guidelines satisfactory (over 90%) • Adherence is suboptimal among specific subgroups of patients: with proximal LAD, triple vessel disease & diabetes or renal failure • Results discussed with staff • Are patients sufficiently informed?
Evaluation of Quality of Elective Surgery for Inguinal Hernia Repair in Adults and in Children at Hadassah Dr. Tal Yemini, Dr. Mahmid Badriah, Dr. Yoav Mintz, Prof. Raphael Udassin, Prof. Avraham Rivkind and Prof. Mayer Brezis Departments of General and Pediatric Surgery, Ein Kerem and Mt Scopus & Center for Quality & Safety, Hadassah Hebrew University Medical Center
Goal & Methods • Evaluation of quality of care for unilateral hernia repair by following criteria: • Overall satisfaction • Pain • Return to activity • Complications • Comparison to literature • Prospective phone survey of • 114 adults (age 14-87) • 102 children (age 2-6)
Satisfaction • Satisfaction was high to very high in 94% of both adults and children; • 88% of adult patients and 95% of parents would recommend having such operation at Hadassah • Problems reported: waiting and relation with staff
Pain & return to activity Results concord with reports in literature About 10% of adults had still more pain after surgery than before and not returned to work after 4-6 weeks. These results are consistent with the notion that patients with minimally symptomatic hernia may not need surgical repair JAMA 2006;295:285.
Rates of Complications confidence interval Reported range varies by site of study & methodology & motive (is it voluntary or mandatory?)
Conclusion Performance of surgical repair at Hadassah is consistent with standards reported in literature We could not find similar reports from other Israeli hospitals Importantly, measurement of rate of infection and feedback to surgeons has recently been shown to be an efficient tool to improve performance and reduce infection rates* * Reduction in infection rates by surveillance with follow-up and feedback. British J of Surgery 2006;93:630-638
Can We Reduce Neurosurgical Shunt Infections? Dr. Ido Paldor, Dr. Zvi Israel, Prof. Colin Block and Prof. Mayer Brezis Departments of Neurosurgery and Infectious Diseases & Center for Quality & Safety, Hadassah Hebrew University Medical Center
Background Hydrocephalus (accumulation of cerebrospinal fluid due drainage obstruction) is a neurosurgical condition treated by insertion of a shunt draining fluid from the ventricles. Infection is a serious complication of shunt insertion, with a high mortality rate. Shunts coated with antibiotics may reduce rate of infection.
Results: rate of shunt infection Intervention Mortality dropped from 50% (in infected cases) to none after intervention
Conclusion Intervention reduced rate of infection from average of 25% to less than 5%, and abolished mortality from infection This may derive from antibiotic-coated shunts and also from surveillance itself, shown to reduce surgical site infections* * Reduced risk of surgical site infections through surveillance in a network. Int J Qual Health Care 2006;18: 127-133
Quality of Reconstruction Surgery after Mastectomy Dr. Ravit Yanco, Dr. Matan Cohen, Dr. Ehud Kleiner, Dr. Helen Green & Dr. Avraham Neuman Department of Plastic Surgery & Center for Quality & Safety, Hadassah Hebrew University Medical Center
Results and Conclusion These results are similar to outcomes reported in the U.S.* and will help make better choice of implant * Reconstructive breast implantation after mastectomy for breast cancer: clinical outcomes in a nationwide prospective cohort study. Arch Surg. 2005;140:1152-1159.
Hand-washing by Medical Staff Dr. Dror Cantrell, Prof. Zvi Stern, Prof. Colin Block & Prof. Mayer Brezis Department of Clinical Microbiology & Center for Quality & Safety, Hadassah Hebrew University Medical Center
Increase in physicians hand-washing by alcohol gel * % of physicians washing hands between patient contacts *p<0.001 * Alcohol-chlorhexidine replaced the gel during 1 week Alcohol Gel Available in Ward
Conclusion • A committee for Infection Prevention at Hadassah is now designing a system-wide intervention including: alcohol gel, education and feedback with periodic monitoring of adherence. • Alcohol gel is more expensive that water & soap but if effective, this may have considerable impact on the difficult and costly problem of cross-infections by bugs increasingly resistant to multiple antibiotics.
Evaluation of performance by a specific surgeon being considered for tenure at Hadassah Physician A performs high-risk, complex operations 2.5 more frequently than other surgeons. Post-surgical length of stay for physician A’s patients is shorter by 3-4 days compared to other high complexity patients (p= 0.01). Patients managed by physician A showed a first-month mortality rate of 1 out of 339 (0.28%) not different from the rate of the rest of the urological team over the same period: 7 out of 2164 (0.32%). The bottom line was that physician A performs at least as well as, and probably even better than the other surgeons of the Urology department.
Progress on Previous Projects • Improved glucose control for hospitalized patients with diabetes • Improvement of palliative care • Patient’s empowerment to improve effectiveness and safety of oral anticoagulation • Perioperative prevention of clots • Improved patient instructions at discharge after hip or forearm fractures
Summary & Conclusion • Diverse projects attempt to make healthcare at Hadassah more patient-centered, more evidence-based and more system-minded. • While in some areas, noticeable improvements have been achieved, it is increasingly apparent that further successes require a systematic mode of monitoring and feedback.
Acknowledgments Prof. Yoel Donchin, Ms. Nurit Porat, Prof. Amir Elami, Dr. Ronny Alcalai, Dr. Mahmid Badriah, Dr. Yoav Mintz, Prof. Raphael Udassin, Prof. Avraham Rivkind, Dr. Zvi Israel, Prof. Colin Block, Dr. Ravit Yanco, Dr. Matan Cohen, Dr. Ehud Kleiner, Dr. Helen Green, Dr. Avraham Neuman, Prof. Zvi Stern, Dr. Rony Braunstein, Dr. Rami Oren, Ms. Lois Gordon, & many other physicians, nurses, pharmacists & students greatly contributed to projects described in this report.