Download
1 / 11
110 likes | 284 Vues
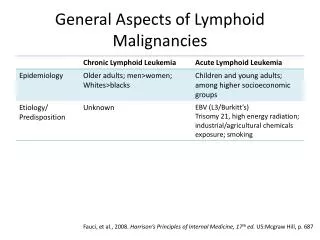
APPROACH TO LYMPHOID MALIGNANCIES. Patient Evaluation of ALL. Careful history and PE CBC Chemistry studies Bone marrow biopsy Lumbar puncture. Prognostic Factors. genetic characteristics of the tumor patient’s age WBC count function of major organs. Patient Evaluation of CLL.

E N D
Patient Evaluation of ALL • Careful history and PE • CBC • Chemistry studies • Bone marrow biopsy • Lumbar puncture
Prognostic Factors • genetic characteristics of the tumor • patient’s age • WBC count • function of major organs
Patient Evaluation of CLL • Careful history and PE • CBC • Chemistry studies • Serumprotein electrophoresis • Bone marrow biopsy • Imaging studies of thechest and abdomen for pathologic lymphadenopathy
Major Prognostic Groups Good prognosis (+) blood and bone marrowinvolvement Intermediate prognosis (+) lymphadenopathy (+) organomegaly Poor prognosis (+) bone marrow failure • Hgb <10g/dL • Platelet count <100,000/iL
Immunologic abnormalities in CLL • Autoimmune hemolytic anemia • Autoimmunethrombocytopenia • Hypogammaglobulinemia
Patient evaluation of Hodgkin’s Disease • Careful history and physical examination • CBC • Erythrocyte sedimentation rate (ESR) • Chemistry studies of major organ function • CT scan of chest, abdomen and pelvis • Bone marrow biopsy
Patient evaluation of Non – Hodgkin’s Disease • Careful history and physical examination • CBC • Erythrocyte sedimentation rate (ESR) • Chemistry studies of major organ function • CT scan of chest, abdomen and pelvis • PET and gallium scan for more aggressive subtypes (e.g.diffuse large B cell lympoma) • Bone marrow biopsy ESR • Serum lactate dehydrogenase (LDH) • β2 – microglobulin • Serum protein electrophoresis
International Prognostic Index for NHL Five clinical risk factors: • Age > 60 years • Serum lactase dehydrogenase levels elevated • Performance status >2 (ECOG) or <70 (Karnofsky) • Ann Arbor stage III or IV • >1 site of extranodal involvement
International Prognostic Index for NHL Patients are assigned a number for each risk factor they have Patients are grouped differently based upon the type of lymphoma For diffuse large B cell lymphoma: 0,1 factor = low risk 35% of cases; 5 – yr survival, 73% 2 factors = low – intermediate risk 27% of cases; 5 – yr survival, 51% 3 factors = high – intermediate risk 22% of cases; 5 – yr survival, 43% 4,5 factors = high risk 16% of cases; 5 – yr survival, 26% For diffuse large B cell lymphoma treated with R – CHOP: 0 factor = very good 10% of cases; 5 – yr survival, 94% 1,2 factors = good 45% of cases; 5 – yr survival, 79% 3,4,5 factors = poor 45% of cases; 5 – yr survival, 55%