Enhancing Lung Cancer Patient Care through the Thoracic Diagnostic Assessment Unit
The Thoracic Diagnostic Assessment Unit (DAU) at Grand River Regional Cancer Centre streamlines the diagnosis and assessment of patients with suspected lung cancer. Our multidisciplinary approach, spearheaded by respirologists and nurse navigators, ensures timely access to care and reduces wait times significantly. From a referral to diagnosis in just 69 days, our program addresses the complex needs of patients through coordinated pathways and evidence-based guidelines. By fostering collaboration with primary care, we empower patients with compassion and support throughout their healthcare journey.

Enhancing Lung Cancer Patient Care through the Thoracic Diagnostic Assessment Unit
E N D
Presentation Transcript
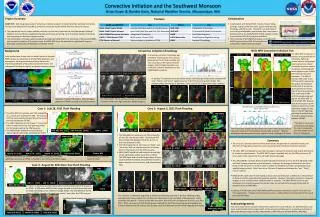
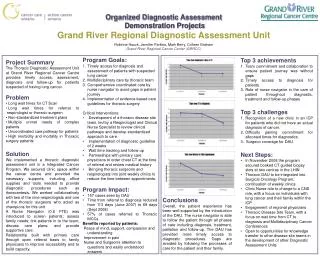
Organized Diagnostic Assessment Demonstration ProjectsGrand River Regional Diagnostic Assessment Unit Robinne Hauck, Jennifer Parkins, Mark Berry, Colleen Graham Grand River Regional Cancer Center (GRRCC) • Program Goals: • 1. Timely access for diagnosis and assessment of patients with suspected lung cancer • Multidisciplinary care by thoracic team • Comprehensive coordinated care by nurse navigator to avoid gaps in patient journey • Implementation of evidence-based care guidelines for thoracic surgery • Critical Interventions: • Development of a thoracic disease site team, led by a Respirologist and Clinical Nurse Specialist to review clinical pathways and develop standardized approach to care • Implementation of diagnostic guideline of 2 weeks • Wait time tracking and follow-up • Partnerships with primary care physicians to order chest CT at the time of referral and review medical history • Bringing thoracic surgeons and respirologists into joint weekly clinics to reduce the time between appointments. • Program Impact: • 157 cases seen by DAU • Time from referral to diagnosis reduced from 113 days (June 2007) to 69 days (Sept 2008) • 57% of cases referred to Thoracic MCCs • Benefits reported by patients: • Peace of mind, support, compassion and understanding • Improvement in pain • Nurse and Surgeon’s attention to questions and easily understood answers • Top 3 achievements • Team commitment and collaboration to ensure patient journey was without gaps • Timely access to diagnosis for patients. • Role of nurse navigator in the care of patient throughout diagnostic, treatment and follow-up phases • Top 3 challenges • Recognition of a new clinic in an ICP for patients who did not have an actual diagnosis of cancer. • Difficulty gaining commitment for allocated times for diagnostics • 3. Surgeon coverage for DAU • Next Steps: • In November 2008 the program secured booked CT guided biopsy slots at two centres in the LHIN • Thoracic DAU to be integrated into Surgical Oncology Program; continuation of weekly clinics • Clinic Nurse role to change to a CNS role, with a focus on individuals with lung cancer and their family within the ICP • Engagement of regional physicians • Thoracic Disease Site Team, with a focus on wait time from CT to diagnosis and Multidisciplinary Cancer Conferences • Open to opportunities for knowledge transfer to other disease site teams in the development of other Diagnostic Assessment Units • Project Summary • The Thoracic Diagnostic Assessment Unit at Grand River Regional Cancer Centre provides timely access, assessment, diagnosis and follow-up for patients suspected of having lung cancer. • Problem • Long wait times for CT Scan • Long wait times for referral to respirologist or thoracic surgeon • Non-standardized treatment plans • Multiple unmet needs of complex patients • Uncoordinated care pathway for patients • High morbidity and mortality in Thoracic surgery patients • Solution • We implemented a thoracic diagnostic assessment unit in a Integrated Cancer Program. We secured clinic space within the cancer centre and provided the necessary supports, including office supplies and tools needed to provide diagnostic procedures such as thoracentesis. We worked collaboratively with two of the nine respirologists and one of the thoracic surgeons who acted as champions for this unit. • A Nurse Navigator (0.6 FTE) was introduced to screen patients; assess family needs; link patients in to the team; discuss care plans; and provide supportive care. • Relationship built with primary care through open referral basis to family physicians to improve accessibility and to build capacity. Conclusions Overall, the patient experience has been well supported by the introduction of the DAU. The nurse navigator is able to follow the patient through all phases of care including diagnosis, treatment, palliation and follow-up. The DAU has provided more timely access to diagnostic procedures. Gaps are avoided by following the processes of care for the patient and their family.