Download
1 / 25
250 likes | 278 Vues
Explore the link between evolution and diseases. Learn how evolutionary biology impacts medicine, defining the norm and understanding mismatches. Dive deep into the concept of "normality" and the implications of ecological niches on health. Discover how an evolutionary perspective can transform medicine. Join the discussion on the evolutionary classification of diseases at the 6th Congress SIBE in Bologna in 2015.

E N D
Evolutionary Classification of Diseases and Similar Conditions Giacinto Libertini (M.D., Independent Researcher) www.r-site.org/ageing, www.programmed-aging.org e-mail: giacinto.libertini@tin.it 6th Congress SIBE – Bologna 2015, August 31 – September 3
What is Evolutionary Medicine? Evolutionary or Darwinian Medicine [1-6] comes into being in 1991 [1], but there are some known forerunners [7] (e.g. [8]) and others not generally cited as forerunners [9, 10]. [1] Williams GC, Nesse RM (1991) The dawn of Darwinian medicine. Quart. Rev. Biol. 66, 1-22. [2] Nesse RM, Williams GC (1994) Why we get sick. Times Books, New York. [3] Stearns SC (ed) (1999) Evolution in health and disease, 1st ed. Oxford University Press, Oxford (UK). [4] Trevathan WR, Smith EO, McKenna JJ (eds) (1999) Evolutionary Medicine. Oxford University Press, New York. [5] Trevathan WR, Smith EO, McKenna JJ (eds) (2008) Evolutionary Medicine: new perspectives. Oxford University Press, New York. [6] Stearns SC, Koella JC (eds) (2008) Evolution in health and disease, 2nd ed. Oxford University Press, Oxford (UK). [7] Trevathan WR, Smith EO, McKenna JJ (2008) Introduction and overview of Evolutionary Medicine. In: Trevathan WR, Smith EO, McKenna JJ (eds) Evolutionary Medicine: new perspectives. Oxford University Press, New York. [8] Eaton SB, Shostak M, Konner M (1988) The paleolithic prescription: a program of diet & exercise and a design for living. Harper & Row, New York. [9] Price WA (1939) Nutrition and Physical Degeneration. Paul B. Hoeber , New York and London. [10] Libertini G (1983) Ragionamenti Evoluzionistici. Società Editrice Napoletana, Naples (Italy). English Edition (2011): Evolutionary Arguments. Azinet Press, Crownsville (USA).
If "Nothing in biology makes sense, except in the light of evolution"[1] is true, why "Nothing in medicine makes sense, except in the light of evolution”[2] should not be true? “Evolutionary Medicine is the enterprise of using evolutionary biology to address the problems of medicine”[3]. Evolutionary Medicine is not an Alternative Medicine (like homeopathy, iridology, ayurvedic medicine, naturopathy, traditional Chinese medicine, energy medicine, etc.) but a Medicine that is more thoroughly scientific in that it involves the concepts of Evolutionism. A medicine that ignored the principles of chemistry, for example, would be partially scientific. Similarly, a medicine that ignores the principles of evolution is partially scientific! [1]Dobzhansky T (1973) Nothing in biology makes sense except in the light of evolution. Am. Biol. Teach. 35:125–9. [2] Varki A (2012) Nothing in medicine makes sense, except in the light of evolution. J. Mol. Med. (Berl.) 90:481-94. [3] Nesse RM, in: Trevathan et al. eds (2008)Evolutionary Medicine: new perspectives. Oxford Univ. Press, New York, Ch. 23.
Some concepts and basic notions are essential for the subsequent exposition 1/3 - The concept of normality in evolutionary terms A normal value, in its statistical meaning, is a value within the reference (or normal) range. It is indispensable to define the reference range as it indicates the “normal” values! E.g., in a mental hospital it is “normal” to be mad and in a cemetery it is “normal” to be dead! For Evolutionary Medicine, in the study of a population we must refer to individuals living in the ecological conditions to which the species is adapted and that will be defined as “normal” conditions.
2/3 - The concept of “mismatch” The concept of “mismatch” is simple but with huge implications: If a species is adapted to a certain range of conditions (including diet, environmental conditions, interrelations with other living beings, etc.), called for brevity “ecological niche”, and that we have defined “normal” conditions, any change in the ecological niche is a potential source of dysfunctions, i.e. diseases, because there is no adaptation to the new conditions [1, 2]. This is defined as "mismatch” [3]. [1] Libertini G (1983) Ragionamenti Evoluzionistici. Società Editrice Napoletana, Naples (Italy). English Edition (2011): Evolutionary Arguments. Azinet Press, Crownsville (USA). [2] Libertini G (2009) Prospects of a Longer Life Span beyond the Beneficial Effects of a Healthy Lifestyle, in: Handbook on Longevity: Genetics, Diet & Disease. Nova Science Publ. Inc., New York. [3] Eaton SB, Shostak M, Konner M (1988) The paleolithic prescription: a program of diet & exercise and a design for living. Harper & Row, New York.
3/3 - Mortality in “normal” conditions The figure shows the life table of a population in “normal” conditions (Ache of Paraguay studied in wild conditions [1]), which mirrors the results of analogous studies (e.g.: [2]). It is noteworthy that, at ages 60 and 70 years, approximately 30% and 18%, respectively, of Ache survived. For Ache, in adults aged 15 to 59 years, the main causes of death were violence (46%), accidents (23%) and infections (24%) The main causes of death in modern populations (heart attacks, diabetes, hypertension, etc.) were absent. Cases of death by cancer were not reported although, in the group aged 60+ years, some rare cases of illness attributed generically to unspecified causes or to “old age” could be the result of a neoplastic disease. [1] Hill K, Hurtado AM (1996) Ache Life History. Aldine De Gruyter, New York. [2] Early J, Peters J (1990) The Population Dynamics of the Mucajai Yanomamo. Academic Press, New York.
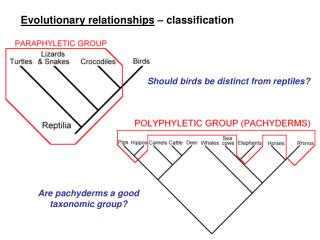
Current classification of diseases and similar phenomena • The International Classification of Diseases, ICD-10 [1], as the preceding ones, classifies the diseases and various similar phenomena following traditional divisions: • - Categories III-XIV mirror the affected organic system (e.g.: circulatory, respiratory, digestive); • - Categories I, II, XV-XVII, XIX mirror specific medical specializations (e.g.: oncology, traumatology); • Categories XVIII, XX-XXII include all other troubles. • - There is NO CODE for ageing, which is considered only a term to summarize an array of distinct degenerative age-related phenomena. The "modern" classification of diseases is pre-Darwinian and follows empirical and customary criteria: in short, it is largely based on the organic system affected or on the competence attributed to some specializations. This traditional type of disease classification mirrors the historical development of medicine and its gradual subdivision in various specializations. It has no rational justification, i.e. it is not based on scientific criteria. [1] ICD-10, WHO 2015.
Category I - Diseases deriving from alterations of the genotype The transfer of genetic information from a generation to the next is imperfect, a fact that is fundamental for the whole evolutionary theory. As these modifications are changes in a very complex system, they are, when not neutral, a likely cause of physiologic dysfunctions. A random modification in a complex structure is a probable cause of breakdown (Fig. 2 from [1]). [1] Libertini G (2009) Prospects of a Longer Life Span beyond the Beneficial Effects of a Healthy Lifestyle, in: Handbok on Longevity: Genetics, Diet & Disease. Nova Science Publishers Inc., New York.
In the wild, for genetic diseases, a disorder caused by a single mutation must have a very small frequency (equilibrium frequency, Ce), determined by the balance between new harmful mutations and selective pressures against these mutations (fig. 1). If a disease may be caused by n different mutations, its frequency will be equal to the summation of n equilibrium frequencies, which is still a small number [1]. A B Figure 1 - A) Equilibrium frequency of a recessive harmful gene (Ce) and phenotypic frequency of the disease caused by it (Pe); B) The same for a dominant harmful gene. Values calculated with a frequency of new mutations equal to 0.00001. For formulas, see [1]. Note that the values of the two Pe are identical (Fig. 3 from [1]). Consequently, it is foreseeable that there is a large number of diseases caused by genetic disorders, each with a limited frequency but with a discrete overall incidence, a prediction confirmed [2]. [1] Libertini G (2009) Prospects of a Longer Life Span beyond the Beneficial Effects of a Healthy Lifestyle, in: Handbook on Longevity: Genetics, Diet & Disease. Nova Science Publishers Inc., New York. [2] Online Mendelian Inheritance in Man. Center for Medical Genetics, Johns Hopkins University (Baltimore, MD, USA), http://www.ncbi.nlm.nih.gov/omim.
Category II - Diseases deriving from alterations of the ecological niche, i.e. consequences of mismatches between adaptation and modified lifestyles As the modifications of the ecological conditions to which a species is adapted are changes in a very complex system, they are, when not neutral, a likely cause of disease. As for genetic diseases, a random modification in a complex order, i.e. a modification of the ecological niche, is a probable cause of disharmony (Fig. 2 from [1]).
There are many diseases deriving from alterations of the ecological niche. The frequency of each of these diseases may be very high and the overall frequency is so high that each person may suffer from various of them. [1] Eaton SB et al. (1988) The paleolithic prescription: a program of diet & exercise and a design for living. Harper & Row, New York. [2] Bragulat E, de la Sierra A (2002) Salt intake, endothelial dysfunction, and salt-sensitive hypertension. J. Clin. Hypertens. (Greenwich) 4, 41-6. [3] Rodriguez-Iturbe B et al. (2007) Pathophysiological mechanisms of salt-dependent hypertension. Am. J. Kidney Dis. 50, 655-72. [4] Morse SA et al. (2005) The heart in obesity-hypertension. Expert. Rev. Cardiovasc. Ther. 3, 647-58. [5] Fredrick DR (2002) Myopia. BMJ. 324, 1195-9. [6] Rose KA et al. (2008) Myopia, lifestyle, and schooling in students of Chinese ethnicity in Singapore and Sydney. Arch. Ophthalmol. 126, 527-30. [7] Wong TY et al. (2000) Prevalence and risk factors for refractive errors in an adult Chinese population in Singapore. Invest. Ophthalmol. Vis. Sci. 41, 2486-94. TO BE CONTINUED …
… CONTINUED [1] Lipworth L et al. (2006) The epidemiology of renal cell carcinoma. J. Urol. 176, 2353-8. [2] Morse SA et al. (2005) The heart in obesity-hypertension. Expert. Rev. Cardiovasc. Ther. 3, 647-58. [3] Eaton SB et al. (1988) The paleolithic prescription: a program of diet & exercise and a design for living. Harper & Row, New York. [4] Fransen E et al. (2008) Occupational noise, smoking, and a high Body Mass Index are risk factors for age-related hearing impairment and moderate alcohol consumption is protective: a European population-based multicenter study. J. Assoc. Res. Otolaryngol. 9, 264-76. [5] Daniel E (2007) Noise and hearing loss: a review. J. Sch. Health 77, 225-31. [6] Viegi G et al. (2006) Epidemiology of chronic obstructive pulmonary disease: health effects of air pollution. Respirology 11, 523-32. [7] Taraseviciene-Stewart L, Voelkel NF (2008) Molecular pathogenesis of emphysema. J. Clin. Invest. 118, 394-402. TO BE CONTINUED …
… CONTINUED [1] Giovino GA (2007) The tobacco epidemic in the United States. Am. J. Prev. Med. 33, S318-26. [2] Clavel J (2007) Progress in the epidemiological understanding of gene-environment interactions in major diseases: cancer. Cancer Res. Biol. 330, 306-17. [3] La Vecchia C et al. (2008) Alcohol and laryngeal cancer: an update. Eur. J. Cancer Prev. 17, 116-24. [4] Janković S, Radosavljević V (2007) Risk factors for bladder cancer. Tumori 93, 4-12. [5] Lipworth L et al. (2006) The epidemiology of renal cell carcinoma. J. Urol. 176, 2353-8. [6] Hart AR et al. (2008) Pancreatic cancer: a review of the evidence on causation. Clin. Gastroenterol. Hepatol. 6, 275-82. [7] Halter F, Brignoli R (1998) Helicobacter pylori and smoking: two additive risk factors for organic dyspepsia. Yale J. Biol. Med. 71, 91-9. [8] Parasher G, Eastwood GL (2000) Smoking and peptic ulcer in the Helicobacter pylori era. Eur. J. Gastroenterol. Hepatol. 12, 843-53. [9] Eaton SB et al. (1988) The paleolithic prescription: a program of diet & exercise and a design for living. Harper & Row, New York. [10] Price WA (1939) Nutrition and Physical Degeneration. Paul B. Hoeber, New York and London. TO BE CONTINUED …
… CONTINUED [1] Trepel F (2004) [Dietary fibre: more than a matter of dietetics. II. Preventative and therapeutic uses][Article in German] Wien. Klin. Wochenschr. 116, 511-22. [2] Arnbjörnsson E (1983) Acute appendicitis and dietary fiber. Arch. Surg. 118, 868-70. [3] Adamidis D et al. (2000) Fiber intake and childhood appendicitis. Int. J. Food. Sci. Nutr. 51, 153-7. [4] Eaton SB et al. (1988) The paleolithic prescription: a program of diet & exercise and a design for living. Harper & Row, New York. [5] National Institutes of Health, USA (2000) Osteoporosis prevention, diagnosis, and therapy. NIH Consens. Statement. 17, 1-45. [6] Janeway C et al. (2001) Immunobiology , 5th ed. Garland Science, New York and London. [7] Kirchner DB (2002) The spectrum of allergic disease in the chemical industry. Int. Arch. Occup. Environ. Health. 75, S107-12. [8] Nesse RM, Williams GC (1994) Why we get sick. Times Books, New York. [9] - Greaves MF (2000) Cancer: The Evolutionary Legacy. Oxford University Press, Oxford (UK). [10] - Adachi M, Brenner DA (2005) Clinical syndromes of alcoholic liver disease. Dig. Dis. 23, 255-63. [11] La Vecchia C et al. (2008) Alcohol and laryngeal cancer: an update. Eur. J. Cancer Prev. 17, 116-24.
Category III - Diseases deriving from ‘extremes’ of the ecological niche (traumas; burns, etc.) “Extremes” are defined the conditions that are beyond the adaptive range of a species. A species cannot be adapted to all possible conditions. E.g., we are not adapted to resist to fire, strong traumas, et cetera. Exposure to conditions for which the species is not (or cannot) be adapted causes troubles or death. This category of diseases is the main cause of death in “normal” conditions [1]. [1] Hill K, Hurtado AM (1996) Ache Life History. Aldine De Gruyter, New York.
Category IV - Diseases deriving from interactions with other living beings (infections, parasitosis, etc.) The number of microbes that are on our epidermis, on our mucosae and in our intestines and elsewhere on or in our body is about TEN TIMES the number of our cells! These microbes are commensals and for many reasons friends of us but in some cases they become our predators. There is a continuous competition among the species, in particular conflictual evolutionary exigencies between an organism and its parasites (bacteria, virus, fungi, worms, etc.). The relationship between an organism and its parasites is analogous to that between a prey and its predators. So, it is predictable that, such as it happens in the prey-predator case, parasites will damage more very young, sick and old individuals and much less healthy and of intermediate ages individuals, to minimise disadvantages and maximise advantages both for hosts and parasites.
Category V - Physiologic phenomena that cause troubles and sufferings, or death: V-1 - Defences against traumas, infections, toxic substances, etc. (i.e. pain, fever, cough, sneezes, nausea, vomit, diarrhoea, iron-deficiency anaemia, etc.) Defences against troubles are often considered as troubles and actively contrasted. In some cases, the “treatment” may be noxious or even deadly. E.g., for iron-deficiency anaemia: “There is convincing evidence that iron deficiency protects against many infectious diseases such as malaria, plague, and tuberculosis as shown by diverse medical, historical, and anthropologic studies.” [1] Iron administration in Polynesian infants increased dramatically gram-negative neonatal sepsis cases and when iron administration was stopped sepses decreased [2]. [1] Denic S, Agarwal MM (2007) Nutritional iron deficiency: an evolutionary perspective. Nutrition 23, 603-14. [2] Barry DM, Reeve AW (1977) Increased incidence of gram-negative neonatal sepsis with intramuscula iron administration. Pediatrics, 60, 908-12. TO BE CONTINUED …
… CONTINUED V-2 - Mental and behavioural troubles as adaptations to particular situations V-3 - Pregnancy, childbirth, puerperium In “normal” conditions, some mental states (e.g., anxiety, mild depression) are often life-saving adaptations to particular situations. Pregnancy, childbirth and puerperium are physiological conditions. Often all these conditions are treated as pathological. Moreover, modifications of the “normal” lifestyle (i.e., alterations of the ecological niche) often transform them in pathological conditions. E.g. the childbirth in aseptic conditions or by Caesarean birth hinders the “normal” colonization of the germ-free bowel of the newborn and this is a cause of serious diseases [1]. [1] Blaser MJ (2014) Missing microbes. Oneworld Book, London.
… CONTINUED V-4 - Phenoptotic phenomena, aging excluded [1] "Phenoptosis is the death of an individual caused by its own actions or by actions of close relatives … and not caused primarily by accidents or diseases or external factors. Phenoptosis is determined, regulated or influenced by genes favoured by natural selection.“ [1] Two examples of phenoptotic phenomena of this category: 1) the "vanishing twin“ (reviewed in 1998 [2]): "... sonograms of women in the first trimester of pregnancy reveal that twins are conceived two to four times more often than they are born; in the majority of cases, the smaller of the two foetuses disappears by the third trimester and is apparently reabsorbed by the mother ...." [3]. 2) “cryptic female choice” [3]. Embryos with too much antigenic homogeneity are more vulnerable to microbial antigenic mimicry and so are eliminated by miscarriage early (more details and references in [1]). [1] Libertini G (2012) Classification of phenoptotic phenomena. Biochem. (Mosc.)77:707-15. [2] Landy HJ, Keith LG (1998) The vanishing twin: a review. Human Reprod. Update 4, 177–83. [3] Hausfater G, Hrdy SB (1984) Infanticide: Comparative and evolutionary perspectives. Aldine, New York. [4] Loisel DA, Alberts SC, Ober C (2008) Functional significance of MHC variation in mate choice, reproductive outcome, and disease risk. In: Stearns, S. C. and Koella J. C. (eds), Evolution in health and disease, 2nd ed. Oxford University Press, Oxford.
… CONTINUED V-5 – Aging Aging, defined as "increasing mortality with increasing chronological age in populations in the wild”, is currently considered as the result of various different degenerative phenomena. A totally alternative interpretation that explains aging as a phenoptotic phenomenon [1-2] has been proposed. It is possible to describe precisely age-related manifestations as the effects of a genetically programmed gradual self-destruction [3]. The evidence and the theoretical arguments against the classic interpretation and in support of the phenoptotic interpretation are overwhelming [4]. It is not possible to really understand aging and a lot of age-related pathologies, both in evolutionary and non-evolutionary terms, if a sound interpretation of aging is not accepted! [1] Libertini G (2012) Classification of phenoptotic phenomena. Biochem. (Mosc.)77:707-15; [2] Skulachev VP (1997)Aging is a specific biological function rather than the result of a disorder in complex living systems: biochemical evidence in support of Weismann's hypothesis. Biochem. (Mosc.) 62:1191-5; [3] Libertini G (2014)Programmed aging paradigm: how we get old. Biochem. (Mosc.) 79(10):1004-16; [4] Libertini G (2015)Non-programmed Versus Programmed Aging Paradigm. Curr. Aging Sci. 8(1):56-68.
Comparison between the different Categories of Diseases and Similar Conditions
Conclusion – Importance and necessity of Evolutionary Medicine The current medicine boasts formidable technical achievements and proclaims that we are increasingly defeating diseases. The reality is quite different. The successes in disease treatments are largely overtaken by the strong increase of many disease frequencies and the average health is getting worse (fig. 1). It is essential to move from the priority given to disease treatment to their prevention based on the fight against their primary causes (and not on screening tests!). For this aim, it is necessary the correct interpretation and classification of diseases. This is a huge goal that clashes with enormous economic interests and many established ideas. But this aim cannot be postponed indefinitely: the preventable deaths and diseases caused by the current irrational organization of the health systems is a load more lethal than that of a world war in progress! Figure 1 - “Growing Sickness. Although people are living longer, they are also living with more chronic conditions, as seen here in data for the developed world.” [1] [1] Vos T et al. (2015) Lancet pii: S0140-6736(15)60692-4. TO BE CONTINUED …
Conclusion – Importance and necessity of Evolutionary Medicine Modern doctors are largely unaware even of the most basic principles of Evolutionism, and do not know or understand Evolutionary Medicine. At the same time, evolutionary biologists do not know or understand the diseases and are unaware of the extreme importance of evolutionism applied to Medicine, not as an ancillary discipline but as the core of a rational organization of a health system that should primarily prevent diseases. It is therefore essential the integration of the knowledge of Evolutionism into the active body of current Medicine, transforming it into Evolutionary Medicine. Important part of this “revolution” is a rational classification of the diseases, based not on the tradition but on a scientific criterion: evolutionism! … CONTINUED
Thanks for your attention This oral presentation is on my personal pages too: www.r-site.org/ageing and you may find it on www.researchgate.net and www.academia.edu (e-mail: giacinto.libertini@tin.it)