Download
1 / 16
440 likes | 4.31k Vues
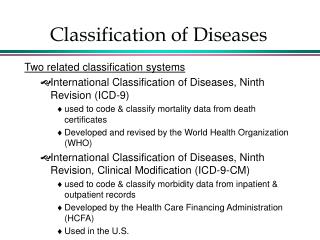
AAP Classification of Periodontal Diseases and Conditions (1999). Gingival Diseases Dental plaque-induced gingival diseases Non-plaque induced gingival lesions Chronic Periodontitis (Slight: 1-2mm CAL; moderate: 3-4mm CAL; severe: >5mm CAL) Localized

E N D
AAP Classification of Periodontal Diseases and Conditions (1999) • Gingival Diseases • Dental plaque-induced gingival diseases • Non-plaque induced gingival lesions • Chronic Periodontitis (Slight: 1-2mm CAL; moderate: 3-4mm CAL; severe: >5mm CAL) • Localized • Generalized (>30% of sites are involved) • Aggressive Periodontitis (Slight: 1-2mm CAL; moderate: 3-4mm CAL; severe: >5mm CAL) • Localized • Generalized (>30% of sites are involved)
AAP Classification of Periodontal Diseases and Conditions (1999) • Periodontitis as a Manifestation of Systemic Diseases • Associated with hematological disorders • Associated with genetic disorders • Not otherwise specified • Necrotizing Periodontal Diseases • Necrotizing ulcerative gingivitis • Necrotizing ulcerative periodontitis • Abscesses of the Periodontium • Gingival abscess • Periodontal abscess • Pericoronal abscess
AAP Classification of Periodontal Diseases and Conditions (1999) • Periodontitis Associated with Endodontic Lesions • Combined periodontic-endodontic lesions • Developmental or Acquired Deformities and Conditions • Localized tooth-related factors that modify or predispose to plaque-induced gingival diseases periodontitis • Mucogingical deformities and conditions around teeth • Mucogingival deformities and conditions on edentulous ridges • Occlusal trauma The Periodontal Disease Classification System of the American Academy of Periodontology - An Update, Journal of Canadian Dental Association, 2002; 66:549-7 Crystal S. Baik
What is Refractory Periodontal Disease • Refractory periodontal disease refers to destructive periodontal diseases in patients who demonstrate continued attachment loss in spite of adequate treatment and proper oral hygiene. • Contributing factors include:type of therapy provided, furcation involvement, microflora, and smoking history. Journal of Canadian Elizabeth Black Dental Association, December 2000
Periodontal Disease and Diabetes • The diabetic state is associated with: • Decreased collagen synthesis • Increased collagenase activity • Altered neutrophil function • Elevated blood sugar levels suppress the host’s immune response and results in: • Poor wound healing • Susceptibility to recurrent infections • Periodontal disease is often considered the 6th complication of diabetes and may place the individual at risk for future diabetic complications *From The Amer Acad of Periodontology, pamphlet "Diabetes and Periodontal Disease", 2002 Prepared by Kristina Fekete
Periodontal Disease & Diabetes BRITTLE DIABETICS: • More susceptible to gingivitis, gingival hyperplasias and periodontitis • More harmful proteins (cytokines) in their gingival tissues • Decreased beneficial proteins (growth factors) interferes with the healing response • Increased levels of serum triglycerides may be related to greater probing depths and attachment loss *From Fedi, The Periodontic Syllabus, 4th ed., 2000 Prepared by Kristina Fekete
Periodontal Disease and Diabetes TREATMENT: • Closely monitor blood glucose levels • Maintenance of meticulous oral hygiene and strict recall appointments • Short appointments in relaxed, non-stressful environment • Have source of oral glucose available • Effective treatment of periodontal infection and reduction of periodontal inflammation are associated with a reduction in the level of glycosylated hemoglobin – the marker of diabetic control *From Little & Falace, Dental Management of the Medically Compromised Patient, 5th ed., 1997 Prepared by Kristina Fekete
Periodontal Treatment and Diabetes -The diabetic patient requires special precautions prior to periodontal treatment -treatment in the uncontrolled diabetic is contraindicated -treatment in the “brittle” diabetic requires prophylactic antibiotics, started 2 days preoperatively (Penicillin VK) and continuing through the immediate post-op period -treatment of the well-controlled diabetic may the same as an ordinary patient
Periodontal Treatment and Diabetes • Protocol for Treatment: • Clinician should make sure that prescribed insulin has been taken, followed by a meal • Morning appointments are appropriate because of optimal insulin levels • Monitor vitals, including blood glucose prior to treatment • Procedures performed may alter the patient’s ability to maintain caloric intake, therefore post-op insulin doses should be altered accordingly • Tissues should be handled as atraumatically and minimally as possible (less than 2 hrs) • Epinephrine should not be used in concentration greater than 1:100,000 due to epinephrine effects on insulin • Diet recommendations should be made to maintain proper glucose balance • Frequent recall and fastidious home oral care should be stressed
Periodontal Treatment and Diabetes • Recent Studies: -Effective treatment of periodontal infection and reduction of periodontal inflammation are associated with a reduction in the level of glycated hemoglobin -Increased serum triglyceride levels in uncontrolled diabetics have been shown to be related to greater attachment loss and probing depths -Therefore…Control of periodontal disease should be an important part of the overall management of the diabetic patient Sources: Carranza and Newman, Clinical Periodontology, 8th ed. Grossi, et al. Treatment of Periodontal Disease in Diabetics Reduces Glycated Hemoglobin. Journal of Periodontology, Vol. 68, No. 8 Chris VanDeven
Smoking and Periodontal Disease • Smoking is a major cause of periodontal disease. • Smokers are 4x as likely to develop periodontitis as non-smokers. • Smoking may be responsible for more than half of the periodontal disease among adults in the U.S. • Up to 90% of refractory periodontitis patients are smokers. References: 1) Tomar, S., Asma, S. ; J Periodontol 2000;71:743-751 2) Johnson GK. Slach NA. Impact of tobacco use on periodontal status. [Review]Journal of Dental Education. 65(4):313-21, 2001 Apr. Graham Smith
Smoking and Periodontal Disease • Smoking may increase levels of certain periodontal pathogens. • Smoking has a negative effect on host response, such as neutrophil function and antibody production. • Smoking has been shown to have a cytotoxic effect on gingival fibroblasts and could slow down wound healing. References: 3) Rota MT.; Tobacco smoke in the development and therapy of periodontal disease: progress and questions. [Review] Bulletin du Groupement International Pour la Recherche Scientifique en Stomatologie et Odontologie. 41(4):116-22, 1999 Oct-Dec. 2) Johnson GK. Slach NA. Impact of tobacco use on periodontal status. [Review]Journal of Dental Education. 65(4):313-21, 2001 Apr. Graham Smith
Smoking and Periodontal Disease • Smoking may be one parameter to use in deciding to treat refractory periodontitis in smokers with a systemic antibiotic therapy directed against smoking-associated periodontal bacteria. • Smoking cessation seems to have a beneficial effect on periodontal health. References: 4) Lie MA. [Smoking as a risk factor for periodontitis]. [Review] [Dutch]Nederlands Tijdschrift voor Tandheelkunde. 106(11):419-23, 1999 Nov. 5) van Winkelhoff AJ. Bosch-Tijhof CJ. Winkel EG. van der Reijden WA. Smoking affects the subgingival microflora in periodontitis.Journal of Periodontology. 72(5):666-71, 2001 May. Graham Smith
What is Periostat? • Doxycycline Hyclate- inhibits collagenase activity and reduces the collagenase activity in gingival crevicular fluid of patients with adult periodontitis • Indicated for use as an adjunct to scaling and root planing to promote attachment level gain and to reduce pocket depths • Periostat is available as a tablet(20mg) to be taken orally two times a day (about an hour before, or two hours after meals). Should be taken with plenty of fluids. • Typical treatments range from 3months to 12months. • www.Periostat.com R.Macnowski
What is Periostat? • Clinical studies have shown that the use of Periostat, along with SC/RP is more effective at regaining attachment level, than treatment with SC/RP alone • Periostat is the first and only therapeutic agent designed to modulate the host response and helps to slow the progression of periodontal disease. • Periostat should be used when traditional SC/RP treatments alone are ineffective, but before surgery is indicated. • www.Periostat.com R. Macnowski
What is Periostat? • Periostat is not an antibiotic- the low dosages of periostat have no detectable effect on bacteria. • Periostat should not be used with children, expecting mothers, nursing mothers, or anyone with a tetracycline hypersensitivity. • Periostat may cause hypersensitivity to sunlight • No reports of tooth staining • May reduce the effect of BCPs • www.periostat.com R.Macnowski