Medicaid Expansion
280 likes | 434 Vues
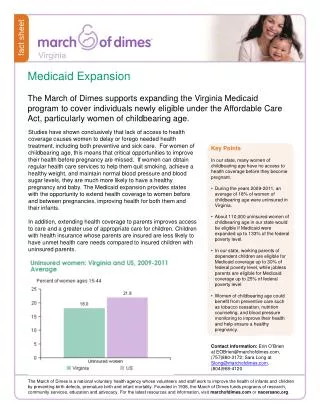
Medicaid Expansion. Jill Beiser, Kathleen Power, & Megan Reid. Problem Identification. Patient Protection and Affordable Care Act, aka Obamacare. Affordable health insurance for ALL! Tax credits Tax breaks Health insurance exchanges Choice of the States - The Problem. Background - Social.

Medicaid Expansion
E N D
Presentation Transcript
Medicaid Expansion Jill Beiser, Kathleen Power, & Megan Reid
Problem Identification • Patient Protection and Affordable Care Act, aka Obamacare. • Affordable health insurance for ALL! • Tax credits • Tax breaks • Health insurance exchanges • Choice of the States - The Problem
Background - Social • Enacted in 1965 • Initially, a medical care extension of programs providing assistance for poor • Emphasis on children, their mothers, disabled, and elderly • Gradually expanded Medicaid’s beneficiaries from 4 million to nearly 60 million (Kaiser Commission, 2011)
Background - Economic • Federal government pays a share of medical assistance expenditures • Determined annually comparing state’s average per capita income level with national income level • Higher per capita income level reimbursed less • Enrollment grown over 7 million since 2007 • Major item in federal and state budget • 3rd largest domestic program in federal • 2nd largest program in most states
Background - Ethical • Ethical issues • Moral foundations, cost containment, public health, and access to care • Primary ethical issue • Distributive justice • Is health care a right or an option?
Background - Legal • Payment reform. • New reimbursement structures. • Access to program participation in Medicaid and health insurance exchanges and products.
Background - Political • Republican vs. Democratic views. • Massachusetts’ formula. • Where does Kansas stand?
Issue Statement How can the federal and state governments implement changes to Medicaid in order to provide adequate health insurance to impoverished citizens without causing the state or federal governments unreasonable debt?
Stakeholders • All U.S. citizens under the age of 65 with family incomes < 133% of the federal poverty level (Medicaid, 2013) • Federal government • States • Taxpayers • Hospitals • Physicians/NP’s/PA’s
Policy Objectives 1) Expand Medicaid coverage to all individuals up to age 65 with incomes <133 % of the federal poverty level 2) Establish policies at the state level that increase funding for Medicaid expansion in line with the ACA. 3) Develop legislation at the federal level and agreements between states to ensure short-term and long-term federal funding for Medicaid expansion
Policy Objectives cont. 4) Structure priorities and policies at the state level that reflect citizens needs and support expanded coverage while remaining financially sound. 5) States periodically update and refine their budget for Medicaid as the nature and cost of healthcare changes in order to maintain the same level of care for their citizens.
Policy Alternatives • Do Nothing Option • Incremental Change Option • Major Change Option
Evaluation Criteria • 1) The probability of states being able to support the financial responsibilities of decision about Medicaid expansion and alternatives. • 2) The efficacy and affordability of proposed plan to the citizens of the United States. • 3) The ability of the plan to meet the healthcare demand of current and future population needs. • 4) Political feasibility for state and federal governments.
Analysis of Option 1: The Do Nothing Option • Criterion 1: States able to support financially • Pro: States avoid relying on federal money • Con: Does not fix or help decrease cost • Criterion 2: Efficacy/affordability to citizens • Pro: Keep tax increases to a minimum and allows states to focus on other priorities • Con: Raise health insurance and decrease insured
Analysis of Option 1: The Do Nothing Option • Criterion 3: Meet healthcare demand • Pro: Decrease strain on primary care providers • Con: Demand for healthcare unchanged • Criterion 4: Political Feasability • Pro: Follows current institutional structure • Government tends to favor status quo over change • Con: Acts against majorly agreed upon belief that healthcare is a broken system
Analysis of Option 2: Incremental Change Option • Criterion 1: States able to support financially • Pro: Allows states to receive some federal funding • Con: If federal funding reneged, states bear burden • Criterion 2: Efficacy/affordability to citizens • Pro: Increases access and minimizes costs • Con: Less money to other priorities and tax increases
Analysis of Option 2: Incremental Change Option • Criterion 3: Meet healthcare demand • Pro: Increased accessibility/affordability and focus on prevention • Con: Further shortage of PCPs, increased strain, decreased hospital productivity • Criterion 4: Political Feasibility • Pro: Allows for shared costs and independence of states • Con: Requires agreement and has less clear guidelines related to federal funding
Analysis of Option 3: Major Change Option • Criterion 1: States able to support financially • Pro: Increases federal funding • Con: Maximizes federal government spending and may fall back onto states • Criterion 2: Efficacy/affordability to citizens • Pro: More money to other state priorities, minimize tax increases, affordable health care • Con: May still lead to tax increases and increases to already insured plans
Analysis of Option 3: Major Change Option • Criterion 3: Meet healthcare demand • Pro: Increase in insured • Con: Does not address shortage of PCPs • Criterion 4: Political feasibility • Pro: Realigns federal and state responsibilities with use of increased federal matching • Con: Requires more stringent funding guidelines and requires agreement
Comparison of Policy Alternatives • Tie between Alternatives 2 and 3 • Alternative 2 is more politically feasible but alternative 3 has stronger ability to meet current/future needs of U.S. citizens • Alternative 3 requires the most funding from federal government but frees states’ resources.
Summary/Recommendations • Medicaid expansion will provide eligibility to all people under 65 with incomes <133% of the (FPL). • Opens up eligibility to Millions of low-income adults without children, low-income parents, children who are now on CHIP • Expected to cover an additional 16 million people by 2019 (Kaiser, 2010).
Recommendations • Alternative 2, the Incremental Change Option is more politically feasible • A systems design would allow for sharing between states and the federal government • Option 2 increases health insurance for millions of people • More focus on prevention means less visits to ER
References • The Advisory Board Company. (2013). Where each state stands on ACA’s Medicaid expansion. Retrieved from http://www.advisory.com/Daily-Briefing/2012/11/09/MedicaidMap • American Public Health Association (2013). Medicaid Expansion. Retrieved March 5, 2013 from http://www.apha.org/advocacy/Health+Reform/ACAbasics/medicaid.htm. • American College of Emergency Physicians. (2011). Ethics of health care reform: Issues in emergency – medicine – An information paper. Retrieved from www.acep.org/Content.aspx?id=80871. • Association of American Medical Colleges. (2010). Physician shortages worsen without increase residency training. Retrieved from https://www.aamc.org/download/153160/data/physician_shortages_to_worsen_without_increases_in_residency_tr.pdf • Galewitz, P. (2012). Study: Nearly a third of doctors won’t see new Medicaid patients. Kaiser Health News. Retrieved February 6, 2013 from http://www.kaiserhealthnews.org/stories/2012/august/06/third-of-medicaid-doctors-say-no-new-patients.aspx • The Heritage Foundation. (2013). Medicaid expansion in Kansas: Impact and cost to taxpayers. Retrieved from http://www.heritage.org/multimedia/infographic/2013/03/medicaid-expansion/kansas. • Holahan, J. (2009). Alternatives for financing Medicaid expansions in health reform. Kaiser • Commission on Medicaid and the Uninsured. Retrieved from http://www.kff.org/healthreform/upload/8029.pdf
References • Kansas Health Institute New Service. (2012). Brownback says no again to health insurance exchanges. Retrieved from: http://www.khi.org/news/2012/nov/08/brownback-says-no-again-health-insurance-exchange/. • Kaiser Commission. (2010). Medicaid coverage and spending in health reform: National and state-by-state results for adults at or below 133% FPL. Retrieved from http://www.kff.org/healthreform/upload/medicaid-coverage-and-spending-in-health-reform-national-and-state-by-state-results-for-adults-at-or-below-133-fpl.pdf • Kaiser Commission. (2011). Medicaid and the uninsured. Retrieved from http://www.kff.org/medicaid/upload/8165.pdf • Kaiser Family Foundation (2012). The Health Reform Law’s Medicaid Expansion: A Guide to the Supreme Court Arguments. Retrieved March 5, 2013 from http://www.kff.org/healthreform/upload/8288.pdf. • Lachman, V. D. (2009). Ethical challenges in healthcare: Developing your moral compass. New York, NY: Springer. • Lachman, V. D. (2012). Ethical challenges in the era of health care reform. Medsurg Nursing 21(4). Retrieved from http://www.nursingworld.org/MainMenuCategories/EthicsStandards/Resources/Ethical-Challenges-in-the-Era-of-Health-Care-Reform.pdf. • Medicaid (2013). HealthCare.gov. Retrieved February 5, 2013 from http://www.healthcare.gov/using-insurance/low-cost-care/medicaid/ • National Association of Public Hospitals and Health Systems (2012). Medicaid expansion benefits everyone. Retrieved February 5, 2013 from http://www.naph.org/Homepage-Sections/Advocate/Medicaid-Expansion-Benefits-Everyone.aspx?FT=.pdf
References • Kaiser Commission. (2011). Medicaid and the uninsured. Retrieved from http://www.kff.org/medicaid/upload/8165.pdf • Nordal, K.C. (2012). Healthcare reform: Implications for independent practice. Professional Psychology: Research and Practice, 43(6): 535-544. • Oberlander, J. (2012). The future of Obamacare. New England Journal of Medicine, 367(2): 2165-2167. • The Patient Protection and Affordable Care Act, 42 U.S.C. 300gg et seq. (2010). Retrieved from http://www.gpo.gov/fdsys/pkg/BILLS-111hr3590enr/pdf/BILLS-111hr3590enr.pdf • Social Security Administration. (2012). Annual statistical supplement to the social security bulletin, 2011 (SSA Publication No. 13-11700). Washington DC. • United States Census Bureau. (n.d.). Health insurance highlights: 2011. Retrieved from http:// www.census.gov/hhes/www/hlthins/data/incpovhlth/2011/highlights.html • U.S. Department of Health and Human Services. (n.d.) Read the Law. Retrieved from http://www.healthcare.gov/law/full/ • U.S. News & World Report (2013). Is Medicaid expansion good for the states? Retrieved February 5, 2013 from http://www.usnews.com/debate-club/is-medicaid-expansion-good-for-the-states • Wilson, M. (2013). Lawmakers urge final answer on Medicaid expansion. State house sound bites. Retrieved February 5, 2013 from http://www.witf.org/state-house-sound-bites/2013/02/lawmakers-urge-final-answer-on-medicaid-expansion-1.php • Wichita Eagle (2013). Eagle editorial: Medicaid expansion boosts state. The Wichita Eagle. Retrieved March 5, 2013 from http://www.kansas.com/2013/02/21/2683996/eagle-editorial-medicaid-expansion.html.