Download
1 / 34
340 likes | 366 Vues
Explore the evolving landscape of cellular therapies for pediatric acute lymphoblastic leukemia, covering presentation, treatment challenges, CART therapy outcomes, and hematopoietic cell transplantation benefits.

E N D
Cellular Therapies for Pediatric Acute Lymphoblastic Leukemia Larisa Broglie, MD MS Assistant Professor of Pediatric Blood and Marrow Transplantation Transplant and Cellular Therapy Meetings February 20, 2019
Objectives • Review Acute Lymphoblastic Leukemia (ALL) – presentation, treatment, and outcomes • Discuss therapy for relapsed ALL and challenges in treatment • Discuss Chimeric Antigen Receptor T-cell therapy (CART) – outcomes and complications • Discuss the expanding landscape of cellular therapy for pediatric leukemias
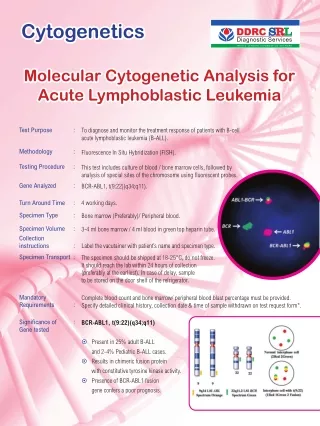
Acute Lymphoblastic Leukemia (ALL) is the most common malignancy in children • Approximately 3,000 new cases per year • Clinical presentation: fever, fatigue, bruising/bleeding, bone pain • Categorized as precursor B-cell ALL (pre-B ALL), or T-cell ALL Pre B-ALL CD19 CD34 CD22 CD10 TdT CD13 Principles and Practice of Pediatric Oncology, Pizzo and Poplack 2015.
Survival for Pediatric B-cell ALL has significant improved Hunger SP, Mullighan CG. N Engl J Med 2015
Challenges remain for patients with relapsed or refractory disease • Almost all patients achieve remission after the first month of chemotherapy • Treatment continues for 3 years for boys and 2 years for girls • Approximately 15-20% of patients eventually relapse • Difficulty in complying with the prolonged, maintenance therapy • High risk features • Aggressive cytogenetic abnormalities
Outcomes depend on location and timing of relapse • Location: • Bone Marrow • Central Nervous System (CNS) • Both • Timing: • Very Early = <18mo from diagnosis • Early = >18mo after diagnosis but <6mo from completion of chemotherapy • Late = >6mo after completing chemotherapy (>36mo from diagnosis) Isolated BM relapse Early Combined BM relapse Early Nguyen K et al. Leukemia. 2008
Hematopoietic Cell Transplantation (HCT) improves outcomes for high risk, relapsed ALL • High risk patients: • very early BM or combined relapse • early BM relapse • Chemotherapy alone resulted in subsequent relapse or death in all patients • HCT improved outcomes with Event Free Survival (EFS) of almost 50% N=58, unrelated donor BMT N=53, chemotherapy Borgmann, A et al. Blood. 2003
Outcomes improved if negative minimal residual disease (MRD) state can be achieved No relapses if MRD negative pre-HCT Survival improves if MRD negative pre-HCT Pulsipherer al. Blood. 2015
Survival after HCT is dependent on remission status 1 CR1 CR2 or greater Induction Failure or Active Disease D'Souza A, Fretham C. CIBMTR Summary Slides, 2017
ALL Summary • Most patients with pre-B ALL achieve sustained remission with chemotherapy • Approximately 15-20% relapse, requiring intensification of therapy and many benefit from stem cell transplantation • Greatest benefit from HCT is when patients have little disease remaining (MRD negative) • Challenges remain for some patients: • Refractory to upfront, standard therapies • Unable to achieve remission after relapse
Immunotherapy – targeting the immune system against leukemia • Hematopoietic Cell Transplantation • Targeted Monoclonal Antibodies (Rituximab) • Bispecific T-cell Engagers (Blinatumomab, Inotuzumab) • Chimeric Antigen Receptor T-cell Therapy (CART) Brown, P. Blood. 2018
What is CART? C • Chimeric • Antigen • Receptor • T-cell • T-cells elicit a cytotoxic response to foreign antigens • Leukemia persists because it evades detection by the immune system • CART harnesses the immune system to fight cancer • Autologous T-cells are manipulated to target leukemia • Primary target is CD19 – a marker on pre-B ALL cells A R T
30 years of progress to bring CART to the bedside 2013: 2 children with refractory ALL, achieve remission 1980-1990s: Altering T-cell receptor can lead to targeted cell killing 2000s: Second Generation CARTs – improved in vitro killing and persistence in mice 1990s: First Generation CARTs – slow tumor growth in mice 2012: Adult studies begin showing promise of CD19 CAR (Seattle, NCI, MSKCC, Penn) 2017: FDA Approves first CART product Grupp et al. New Eng J Med. 2013 Maude, S et al. New Eng J Med. 2014
Creating autologous T-cells to target leukemia Infusion: Of CAR T-cells into patient Leukapheresis: Collect T-cells Growth: Of T-cells expressing the Chimeric Receptor Viral Transduction: Chimeric receptor transferred into T-cells Shubert et al, Human Gene Therapy. 2016; Frey, NV and Porter, DL. Am J Hematol. 2016
The evolution of Chimeric T-cell Receptors Monoclonal Antibody Transmembrane Domain Co-stimulatory Domain CD3ζ Park JH and Brentjens RJ. Blood. 2015
Are all CARTs created equal? • T-cell Targets • CD19 • Others (CD22, CD20, CD123, CD33, GD2) • Costimulatory Domains • 4-1BB • CD28 • Virus Transduction • Lentivirus • Retrovirus
CAR T-cells induce targeted leukemia cell death T-cell Leukemia Chimeric T-cell Receptor CD 19 Apoptosis
https://www.chop.edu/news/five-years-later-first-pediatric-recipient-car-t-cell-therapy-remains-cancer-freehttps://www.chop.edu/news/five-years-later-first-pediatric-recipient-car-t-cell-therapy-remains-cancer-free
CART therapy leads to high rates of CR • N=30 children and adults with pre-B ALL • 80% of patients had detectable leukemia prior to infusion • 90% achieved complete remission • Only 7 of these patients later relapsed • 6 month EFS = 67%, OS = 78% 20 Maude, S et al. New Eng J Med. 2014
Results were validated in an international study • International trial • N=75 received CART infusion • 81% of patients achieved remission • 59% relapse free survival at 12mo • 22 patients relapsed, 68% were CD19 negative at time of relapse Maude et al. NEJM. 2018
Unique Complications of CART • Hypogammaglobulinemia (low IgG levels) • CD19 is a normal marker on B-cells • Can be a marker of CART persistence • Treatment with IV immunoglobulin • Cytokine Release Syndrome • Neurotoxicity (Immune Effector Cell-Associated Neurotoxicity Syndrome)
Cytokine Release Syndrome • 10yo female receives CART infusion after she fails to respond to chemotherapy for her relapsed B-cell ALL • 3 days after CART infusion, she has a high fever to 40oC • She is started on antibiotics but her blood pressure becomes unstable. She is hypotensive with blood pressures of 70/30s • She is given IV fluid but requires escalating vasopressors • She now requires oxygen supplementation • Due to concern for Cytokine Release Syndrome, she is give a dose of Tocilizumab and she clinically improves
CRS – potentially life threatening systemic inflammation • Due to a cytokine release, predominantly mediated by IL-6 • Approximately >75% of patients experience CRS • Severe, life threatening CRS occurs in 27-44% • Increased risk of severe CRS with: • higher CART cell doses • higher disease burden • concurrent infection • Treatment: • Supportive Care • Anti-IL6 therapy (Tocilizumab, Siltuximab) • Try to avoid steroids if possible as may impair CART cells Lee et al. ASBMT Consensus Guidelines. Biol Blood Marrow Transplant. 2018
CRS Grading – ASBMT Consensus Guidelines Lee et al. ASBMT Consensus Guidelines. Biol Blood Marrow Transplant. 2018
Immune Effector Cell-Associated Neurotoxicity • 13yo male received CART infusion 10 days ago for refractory B-cell ALL • He had CRS requiring a brief ICU stay but improved, and was preparing for discharge home • But, he began complaining of headaches • He worsened and was unable to answer questions or talk; he is less awake and less alert • He was monitored closely but had no seizure or evidence of cerebral edema • He gradual improved over the next weeks with supportive care and rehab
Neurotoxicity can cause cerebral edema and death • Estimated to occur in 25-50% of patients • Headaches can be non-specific • Hallmark symptom is aphasia • Can progress to motor weakness, seizure, cerebral edema and death • The pathophysiology of neurotoxicity is not well understood. • Treatment remains supportive care Lee et al. ASBMT Consensus Guidelines. Biol Blood Marrow Transplant. 2018
Neurotoxicity Grading – ASBMT Consensus Guidelines • Grading scales available for adults and children ≥12yo: • Level of consciousness • Motor findings • Seizure • Increased intracranial pressure • <12yo use Cornell Assessment of Pediatric Delirium: • Eye contact • Communication • Activity • Response to others Lee et al. ASBMT Consensus Guidelines. Biol Blood Marrow Transplant. 2018
Relapse can occur after CART infusion • Relapse can still occur after CART • Relapse can be either: • CD19 positive • CD19 negative • CD19 positive relapse from poor persistence of CART • CD19 negative relapse from new mutations in the leukemia that is no longer recognized by CART
FDA Approval of first 2 CART agents • Tisagenlecleucel • Aka Kymriah • Novartis • $475,000 • Approved for pediatric patients with of refractory or 2nd or later relapse of B-cell ALL • Axicabtagene • Aka Yescarta • Kite Pharma • $373,000 • Approved for adults with relapsed or refractory large B-cell lymphoma
This is just the beginning Wells Fargo Securities Conference, November 2017
More Than Just CARTs • Allogeneic CARTs • CARTs for solid tumors • Tumor specific T-cells • Natural Killer CARTs • And more…
Thank you CIBMTR and the Cellular Therapy Forms Committee • Marcelo Pasquini • Bronwen Shaw • Janet Bruner-Grady • Tiffany Hunt • And more Patients and families Columbia University Pediatric Blood and Marrow Transplant • Prakash Satwani • Monica Bhatia • Diane George • Jim Garvin Data Managers and Research Support Staff