Download
1 / 1
10 likes | 269 Vues
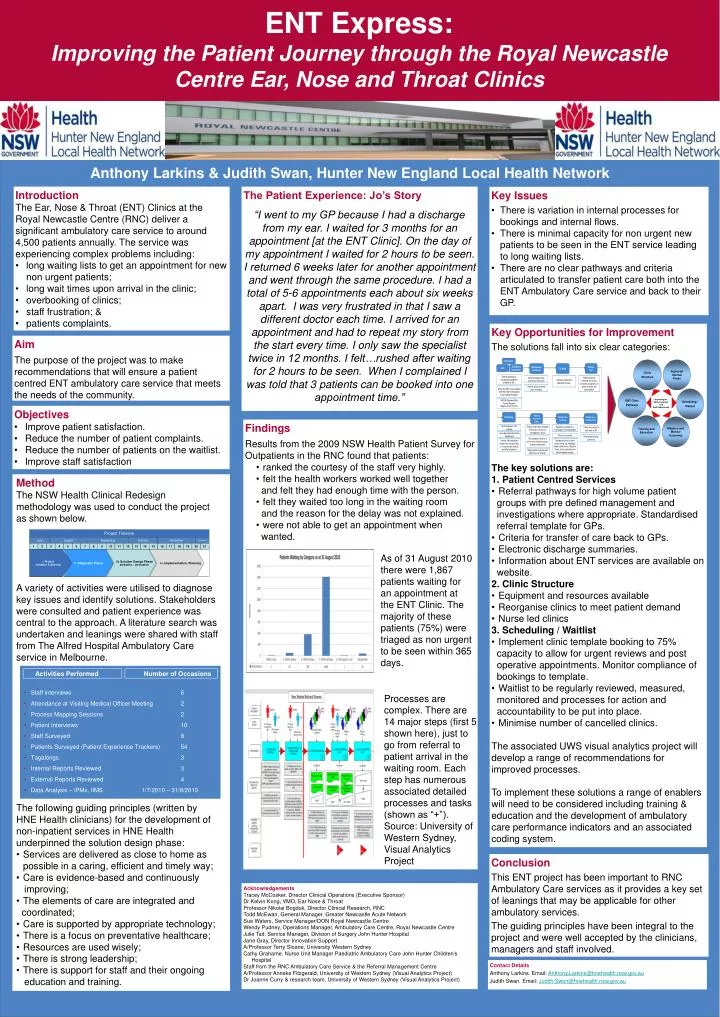
Project Timeline. July. August. September. October. November. December. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. i. Project Initiation & Start-up. ii. Diagnostic Phase. iii. Solution Design Phase 20/9/2010 – 25/10/2010.

E N D
ProjectTimeline July August September October November December 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 i. Project Initiation & Start-up ii. Diagnostic Phase iii. Solution Design Phase 20/9/2010 – 25/10/2010 iv. Implementation, Planning ENT Express: Improving the Patient Journey through the Royal Newcastle Centre Ear, Nose and Throat Clinics Anthony Larkins & Judith Swan, Hunter New England Local Health Network • Introduction • The Ear, Nose & Throat (ENT) Clinics at the • Royal Newcastle Centre (RNC) deliver a • significant ambulatory care service to around • 4,500 patients annually. The service was • experiencing complex problems including: • long waiting lists to get an appointment for new non urgent patients; • long wait times upon arrival in the clinic; • overbooking of clinics; • staff frustration; & • patients complaints. The Patient Experience: Jo’s Story “I went to my GP because I had a discharge from my ear. I waited for 3 months for an appointment [at the ENT Clinic]. On the day of my appointment I waited for 2 hours to be seen. I returned 6 weeks later for another appointment and went through the same procedure. I had a total of 5-6 appointments each about six weeks apart. I was very frustrated in that I saw a different doctor each time. I arrived for an appointment and had to repeat my story from the start every time. I only saw the specialist twice in 12 months. I felt…rushed after waiting for 2 hours to be seen. When I complained I was told that 3 patients can be booked into one appointment time.” • Key Issues • There is variation in internal processes for bookings and internal flows. • There is minimal capacity for non urgent new patients to be seen in the ENT service leading to long waiting lists. • There are no clear pathways and criteria articulated to transfer patient care both into the ENT Ambulatory Care service and back to their GP. • Key Opportunities for Improvement • The solutions fall into six clear categories: • The key solutions are: • 1. Patient Centred Services • Referral pathways for high volume patient • groups with pre defined management and • investigations where appropriate. Standardised • referral template for GPs. • Criteria for transfer of care back to GPs. • Electronic discharge summaries. • Information about ENT services are available on • website. • 2. Clinic Structure • Equipment and resources available • Reorganise clinics to meet patient demand • Nurse led clinics • 3. Scheduling / Waitlist • Implement clinic template booking to 75% • capacity to allow for urgent reviews and post • operative appointments. Monitor compliance of • bookings to template. • Waitlist to be regularly reviewed, measured, • monitored and processes for action and • accountability to be put into place. • Minimise number of cancelled clinics. • The associated UWS visual analytics project will • develop a range of recommendations for • improved processes. • To implement these solutions a range of enablers • will need to be considered including training & • education and the development of ambulatory • care performance indicators and an associated • coding system. Aim The purpose of the project was to make recommendations that will ensure a patient centred ENT ambulatory care service that meets the needs of the community. • Objectives • Improve patient satisfaction. • Reduce the number of patient complaints. • Reduce the number of patients on the waitlist. • Improve staff satisfaction • Findings • Results from the 2009 NSW Health Patient Survey for Outpatients in the RNC found that patients: • ranked the courtesy of the staff very highly. • felt the health workers worked well together • and felt they had enough time with the person. • felt they waited too long in the waiting room • and the reason for the delay was not explained. • were not able to get an appointment when • wanted. • Method • The NSW Health Clinical Redesign • methodology was used to conduct the project • as shown below. • A variety of activities were utilised to diagnose • key issues and identify solutions. Stakeholders • were consulted and patient experience was • central to the approach. A literature search was • undertaken and leanings were shared with staff • from The Alfred Hospital Ambulatory Care • service in Melbourne. • The following guiding principles (written by • HNE Health clinicians) for the development of • non-inpatient services in HNE Health • underpinned the solution design phase: • Services are delivered as close to home as possible in a caring, efficient and timely way; • Care is evidence-based and continuously • improving; • The elements of care are integrated and • coordinated; • Care is supported by appropriate technology; • There is a focus on preventative healthcare; • Resources are used wisely; • There is strong leadership; • There is support for staff and their ongoing • education and training. As of 31 August 2010 there were 1,867 patients waiting for an appointment at the ENT Clinic. The majority of these patients (75%) were triaged as non urgent to be seen within 365 days. Processes are complex. There are 14 major steps (first 5 shown here), just to go from referral to patient arrival in the waiting room. Each step has numerous associated detailed processes and tasks (shown as “+”). Source: University of Western Sydney, Visual Analytics Project Conclusion This ENT project has been important to RNC Ambulatory Care services as it provides a key set of leanings that may be applicable for other ambulatory services. The guiding principles have been integral to the project and were well accepted by the clinicians, managers and staff involved. Acknowledgements Tracey McCosker, Director Clinical Operations (Executive Sponsor) Dr Kelvin Kong, VMO, Ear Nose & Throat Professor Nikolai Bogduk, Director Clinical Research, RNC Todd McEwan, General Manager, Greater Newcastle Acute Network Sue Waters, Service Manager/DON Royal Newcastle Centre Wendy Pudney, Operations Manager, Ambulatory Care Centre, Royal Newcastle Centre Julie Tait, Service Manager, Division of Surgery John Hunter Hospital Jane Gray, Director Innovation Support A/Professor Terry Sloane, University Western Sydney Cathy Grahame, Nurse Unit Manager Paediatric Ambulatory Care John Hunter Children’s Hospital Staff from the RNC Ambulatory Care Service & the Referral Management Centre A/Professor Anneke Fitzgerald, University of Western Sydney (Visual Analytics Project) Dr Joanne Curry & research team, University of Western Sydney (Visual Analytics Project) Contact Details Anthony Larkins. Email: Anthony.Larkins@hnehealth.nsw.gov.au Judith Swan. Email: Judith.Swan@hnehealth.nsw.gov.au