Download
1 / 42
430 likes | 665 Vues
Disorders of the Ear, Nose, Throat & Mouth. Chapter 11 Pathology. EARS. Otitis Externa- a painful inflammation of the membranous lining of the auditory canal and/or contiguous structures. Refers to acute and chronic inflammatory process It may be diffuse or localized

E N D
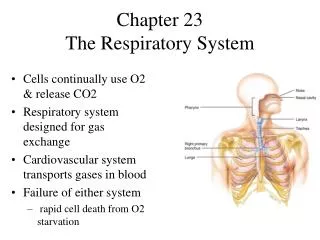
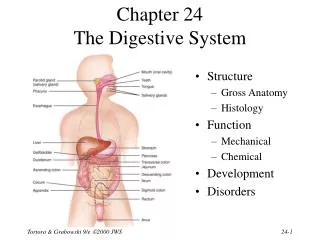
Disorders of the Ear, Nose, Throat & Mouth Chapter 11 Pathology
EARS • Otitis Externa- a painful inflammation of the membranous lining of the auditory canal and/or contiguous structures. • Refers to acute and chronic inflammatory process • It may be diffuse or localized • Is largely benign and self-limiting • Invasive otitis externa is a potentially life threatneing situation
EARS • OE continued • Epidemiology • 10-20% more common in the summer months • Patho- inflammation is most commonly caused by microbial infection. Colonization of the external ear is prevented immune and anatomic mechanisms
EARS • Management and Treatments • Pain meds • Heat or ice • Keep dry- no swimming for 7 days • Treatment for basic OE • Irrigation if indicated • Pain drops • Antibiotic drops • Ciprodex, Floxin Cortisporin • May need a wick if very swollen
EARS • Otitis Media- OM- inflammation of the structures in the middle ear. • Otitis media with effusion –OME involves the transudation of plasma from middle ear blood vessels leading to chronic fluid; this can be chronic • Acute Otitis Media-AOM is infection in the middle ear
EARS • OM • Epidemiology • Accounts for 2-3% of all family practice office visits. Number of visits increases in the winter. More common in colder weather and in children. • Contributing factors include; allergies, rhinitis, pharyngitis due to swelling of upper airway membranes. Most common factor is upper airway infections (colds), caused by many different viruses. • Influenza, RSV, pneumovirus, adenovirus
EARS • OME symptoms • Stuffiness, fullness, decreased hearing, pain is rare, may have popping. Rarely vertigo • Usually a history of recent URI, allergies
Rhinitis • Rhinitis or coryza –inflammation of the nasal mucosa with congestion, rhinorrhea, sneezing, pruritus, post nasal drip • Allergic • Seasonal or perennial • Nonallergic • Infectious, irritant related, vasomotor, hormone-related, associated with medication, or atrophic • May be chronic or acute • Most common types • Viral • Perennial (hay fever)
Rhinitis • Epidemiology/Causes • Actual prevalence is undocumented, but is very common • Occurs at least as much as the common cold • Estimated 40-50 million American adults suffer • Seasonal allergic rhinitis parallels pollen production fall/spring • Allergy occurs in all age groups • Most common in adults 30-40 years • Non allergic rhinitis may be acute or chronic • Chronic maybe associated with bacterial sinusitis
Rhinitis • Rhinitis – symptoms • Viral-malaise, HA, substernal tightness, rare fever, sneezing and coughing • Allergic-itching of all upper air way mucosa, watery eyes, sore throat, sneezing, coughing • Vasomotor-watery nasal discharge, nasal speech, mouth breathing, nasal obstruction that switches sides
Rhinitis • Treatments • Allergic rhinitis • Avoid the triggers • Antihistamines • Allegra, Claritin, Clarinex, Zyrtec, Astelin • Nasal steroids • Flonase, Nasonex, Nasacort • Leukotriene receptor antagonists • Singular • Desensitizing immunotherapy • Atrophic- bacitracin to nares, saline, irrigation
Sinusitis • Sinusitis is an inflammation of the mucous membranes of one or more of the paranasal sinuses; frontal, sphenoid, posterior ethmoid, anterior ethmoid, and maxillary • Acute-abrupt onset of infection and post-therapeutic resolution lasting no more than four weeks • Subacute with a purulent nasal discharge persist despite therapy, lasting 4-12 weeks • Chronic, with episodes of prolonged inflammation with repeated or inadequately treated acute infection lasting greater than 12 consecutive weeks
Sinusitis • Clinical presentation • Gradual onset of symptoms • Pain over the affected sinus, with increasing pain • Pain is worse with coughing • Area of pain corresponds the sinus affected • Develop over at least 2 weeks of URI symptoms • Nasal congestion, runny nose, pressure, cough, sore throat, eye pain, malaise, and fatigue, headache, cough, fever
Sinusitis • Sinusitis Management • Usually viral • Supportive care is most helpful • Sinus rinse • Few meds are helpful • Sudafed, nasal spray, expectorants, • Rarely use steroids or antihistamines • Localized sinus infections are self limited
Sinusitis • Sinusitis patient education • Should focus on the worsening of symptoms • Avoid all contributing factors • Smoke, allergens, antihistamine • Increase fluids
Pharyngitis • Pharyngitis and tonsillitis are generalized inflammatory process of both infectious and non infectious etiology • Most cases are viral and self-limiting • Most cases of pharyngitis are contagious • All cases of tonsillitis are contagious
Pharyngitis • Testing • Viral throat swab cultures are used to detect herpes virus as well other viral infections… • Tzanck smear of a exudate is used to detect HSV, and herpes zoster • Blood test may be used for viruses • HSV, EBV, CMV • Candida – KOH potassium hydroxide- looking for hyphal yeast • Mono spot for mono • CBC for infectious pharyngitis • X-ray may be needed to assess for abscess
Pharyngitis • Management depends on the cause • Home care with symptom management • Voice rest, humidification, saline, viscous Xylocaine, gargles, cool mist, lozenges, sprays, Acetaminophen, codeine, warm compresses for lymph nodes • Antibiotics for bacterial causes • See therapeutics handout • Antifungal for candida • Diflucan, nystatin • Be sure and assess immune status if no known cause is found • Viral illnesses • May use antivirals in some cases- IE; Flu- use Tamiflu • Abscess- hospital IV antibiotics and maybe surgery
Temporomandibular Joint (TMJ) Disease • TMJ is a collective term that refers to disorders affecting the masticatory musculature and associated structures. Sometimes know as temporomandibular disorder. TMD is a cluster or related disorder that have many features in common. • The most common is pain in the muscles of mastication, the preauricular and the TMJ • Is a sub classification of musculoskeletal disorder
Temporomandibular Joint (TMJ) Disease • Epidemiology • 75% of people have at least one sign of joint dysfunction and 33% have at least one symptom, like face pain • Only about 5% are in need of treatment • Differentiate contributing factors • Predisposing factors- increase the risk • Initiating factors- cause the onset • Perpetuating factors- interfere with healing
Temporomandibular Joint (TMJ) Disease • Symptoms • Pain in the preauricular area/or TMJ • Pain, jaw noise, ear symptoms, rarely jaw dislocation • Chewing aggravates • Pain in face or head • Dull pain in temple are • Tinnitus • Sinus symptoms • FB sensation in ear canal • Decreased hearing • Neck or shoulder pain • Visual disturbance • Limited jaw opening • Jaw popping
Temporomandibular Joint (TMJ) Disease • Questionnaires for screening- Example questions • Do your jaws make noise • Does using your jaw cause you pain • Have you had jaw joint problems before • Does you jaw ever get stuck • Is opening your mouth difficult or cause pain • With ringing in the ear does opening or closing you mouth change the sound • Do you have frequent headaches, neck aches, or tooth aches
Temporomandibular Joint (TMJ) Disease • Physical finding • Complete exam to exclude other problems • Observation of gait, balance, unusual habits • Palpate the muscles of mastication using bimanual technique • Start with the mouth closed then open
Temporomandibular Joint (TMJ) Disease • Management • Involves understanding and treating the whole patient • Goals for management- reduction of pain, restorations of acceptable function • Initial TX designed to be palliative and promote healing, with self-help techniques and pharmacotherapy • Adjustment of diet • Education and alteration of oral habits (gum chewing) • ICE/ HEAT • Medications such as pain meds, anti-inflammatory meds, injection of trigger points • Most care will be given by the specialist
TMJ • Follow up and referral • Refer to a specialist is best idea for real TMJ disease
Gingivitis • Inflammation of the gingiva • It may be characterized by edema, erythema, bleeding, and occasionally pain • Gingivitis is usually reversible with appropriate therapy
Periodontitis • An inflammatory disease of the supporting tissues of the teeth caused by specific microorganisms or groups of specific microorganisms, resulting in progressive destruction of the periodontal ligament and alveolar bone with pocket formation, recession, or both.
Oral Trauma What happened Tooth/jaw/lip/tongue hurt What hit you How long ago Where are the teeth
Oral Trauma Teeth Avulsed (knocked out, loose) Fractured Chipped Intrusion Jaw/face: feel for “crunchy” sensation Mucosal/tongue injury
Oral Trauma Teeth Avulsion Primary teeth Out, leave out Loose, straighten or is very loose remove Permanent teeth Out, leave out, wash gently, tooth kit Loose, leave alone Fracture, keep fragment, store as above
Oral Trauma Tongue • Well approximated, nothing • Bleeding direct pressure with gauze • Gaping need repair Mucosal • Well approximated, nothing • Gaping and vermillion border need repair
Oral Trauma Dental injuries Dentist for most injuries Baby teeth may need nothing Tongue/Mucosa Most need nothing Doctor if gaping or severe bleeding
Nose Bleeds How much blood, how long What has been done to stop bleeding Trauma Blunt Picking Upper respiratory infection/Allergies History of Bleeding
Nose Bleeds Nose Fracture (usually at bridge) Active bleeding Which side? Always the same? Throat Neurologic Vision
Nose Bleeds Pinch x 10-20 minutes Ice Nose plugs Don’t blow nose Afrin if available No picking