Download
1 / 78
880 likes | 1.25k Vues
Guidelines To Effectively Manage Perioperative Glycemic Management. Carol Manchester, MSN, ACNS, BC-ADM, CDE Diabetes Clinical Nurse Specialist University of Minnesota Medical Center University of Minnesota Amplatz Children’s Hospital September 26, 2013. Perioperative Hyperglycemia.

E N D
Guidelines To Effectively Manage Perioperative Glycemic Management Carol Manchester, MSN, ACNS, BC-ADM, CDE Diabetes Clinical Nurse Specialist University of Minnesota Medical Center University of Minnesota Amplatz Children’s Hospital September 26, 2013
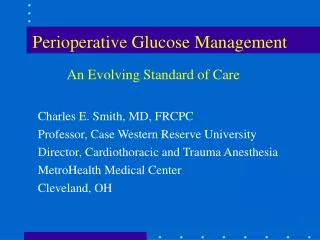
Perioperative Hyperglycemia Adapted from Anesthesiology, 110: 2, Feb. 2009; Lipshutz, M., Gropper, M. Patient Anesthesia Metabolic Stress Critical Illness ↓ Insulin Secretion ↑ Insulin Resistance ↑Counterregulatory Hormones ↑Gluconeogenesis ↓Glucose Utilization Perioperative Hyperglycemia Impaired Chemotaxis and Phagocytosis ↑ Expression of adhesion molecules ↓ Complement Function ↓ Vasodilation Impaired Nitric Oxide Generation ↑ Inflammation Vulnerability to Infection, Multi-Organ System Dysfunction →
Perioperative Phases • Preoperative • Scheduled • Who gives instructions? • Same Day or admission ? • Preadmission process? • History and Physical • Who takes the information? • Are they familiar with the patient? • Medication Reconciliation • Laboratory and Diagnostic Findings • A1C • Intraoperative • Anesthesia • Surgeon • Postoperative • Surgical orders • Medical consult ?
Basal Bolus Blood Glucose NPO Dextrose Source
Conventional Practice Preoperatively • Insulin • Hold AM dose • Give 50% of the basal insulin • AM dose • Night before • Stop infusion pump at midnight • Nutrition and Fluids • Patient is NPO • IV Access ? • Do not administer any IV fluids with dextrose containing solution; NS, LR • Point of Care Values • Glycosylated Hemoglobin A1C • Last BG value obtained HS the night before • Value on call to OR and handed off ?
Conventional Practice Intraoperatively • Insulin • Intravenous insulin infusion • Correction bolus of Regular Insulin, IV • Ambulatory insulin infusion pump on/off? • Nutrition and Fluids • NPO • NS, LR • Point of Care Values • Frequency of glucose monitoring • Arterial line, finger stick, venous sample • Antiemetics and other Medications • Utilization of Dexamethasone • Hypoglycemia Prevention
Conventional Practice Postoperatively • Insulin • IV insulin infusion on/off ? • Correction scale only • Nutrition and Fluids • Clears when awake, alert • NPO • Possible enteral feeding to start at 10 ml. / hr. • NS, LR, 0.45% NS, D5.0.45% NS • Point of Care Values • Immediately in PACU, q 4 hr., q 6 hr., not ordered? • Pharmaceutical Agents • Antibiotics • Vasopressors • Steroids • Concomitant Therapies • Transfusions • Oxygen
What evidence exists? • Stress induced hyperglycemia • Blood glucose > 200 mg/dL in the absence of known diabetes • More common in elderly • Results primarily from the release of • Counterregulatory hormones • Inflammatory cytokines Coursin, DB et al. Critical Care Medicine 32: S 117; 2004
Neurologic Alterations Due to Hyperglycemia • Individuals with a known diagnosis of DM as well as those without DM who are hyperglycemic have increased morbidity and poor clinical outcomes after stroke compared to normoglycemic individuals • Hypothesis that the elevated BG causes intracranial acidosis and exacerbation of neuronal edema initiated by anoxia Anderson, RE et al. Stroke 30: 160; 1999 DeCrespigng AS et al: Stroke 30: 2212; 1999
Hyperglycemia and Dexamethasone • Dexamethasone administered intraoperatively for craniotomy • BG concentration changes were evaluated for 12 hr. in 34 patients without dx of DM • Compared patients who received Dexamethasone 10 mg IV on induction and 4 mg IV 6 hr. later to group with no dexamethasone administered.
Hyperglycemia and Dexamethasone • Peak BG occurred 8-10 hr. after induction • The duration of the surgery had a positive correlation • Recommendations • Maintain BG in patients at risk for ischemic brain injury at 80-150 mg/dL. • Monitor BG for minimum of 12 hr. in individuals without DM having neurosurgery with Dexamethasone administration Lukins, MB et al. Anesthesia Analgesia 100: 1129, 2005.
Abdominal Surgery and Dexamethasone Administration • Study compared the BG profile of patients with type 2 DM and without a dx of DM following Dexamethasone 10 mg • BG increased in both groups of subjects • More pronounced effects • Poorly controlled DM • Obesity Hans, P et al. British Journal of Anaesthesia 2006, 97: 164-70
The Stamford Hospital Experience After institution of Protocol: • Mean glucose value decreased from 152.3 to 130.7 mg/dL • Percentage of glucose values ≥ 200 mg/dL decreased 56.3% • No significant change in hypoglycemia • Development of new renal insufficiency decreased 75% • Number of patients requiring transfusion of packed red blood cells decreased 18.7% • Hospital mortality decreased 29.3% • Length of stay in ICU decreased 10.8% ______________________________________________________ KRINSLEY JS. Effect of Intensive Glucose Management Protocol on the Mortality of Critically Ill Adult Patients. Mayo Clin Proc. 2004; 79: 992-1000.
Hyperglycemia in Hospitalized Medical/Surgical Patients • A single blood glucose level >220 mg/dL on the first post-op day resulted in a 2.7 times higher infection rate in diabetic patients (1) • A significant reduction in daily blood sugar value (125 ± 36 mg/dL vs 179 ± 61 mg/dL) reduced nosocomial infection rate by approximately 30%; including reduction in intravascular device, blood stream, and surgical site infection (2) 1POMPOSELLI JJ. et al. Early Post-operative Glucose Control Predicts Nosocomial Infection Rate in Diabetic Patients. J Parenter Enteral Nutr. 1998; 22: 77-81. 2PERDRIZET GA. et al. Reduction of Hyperglycemia and Nosocomial Infections in a General Surgical Intensive Care Unit. Abstract (2004) from New England Surgical Society. Available at: http://www.nesurgical.org/abstracts/2004/4.cgi. Accessed July 3, 2006.
Tight Glycemic Control An Investment in Enhanced Outcomes and Resource Utilization • For each 50 mg/dL increase in blood glucose in patients with diabetes undergoing CABG there was an additional 0.76-day length of stay (an incremental hospital cost of $1,769) (1) • The use of a diabetic team consultation resulted in 56% reduction in length of stay for a cost reduction of $2,353 per patient (2) 1ESTRADA ES. et al. Outcomes and Perioperative Hyperglycemia in Patients with or without Diabetes Mellitus Undergoing Coronary Artery Bypass Graft. Ann Thorac Surg. 2003; 75: 1392-1399. 2LEVETAN CS. et al. Impact of Endocrine and Diabetic Team Consultation on Hospital Length of Stay for Patients with Diabetes. Am J Med. J1995; 99: 22-28.
Tight Glycemic Control An Investment in Enhanced Outcomes and Resource Utilization Columbus Regional Medical Center, Columbus, GA • 1997: Net cost savings to the hospital from reduced LOS and reduction in unreimbursed recidivistic admissions was $342,166 • 1998: Total savings increased to more than $630,000 LEICHTER SB. et al. The Business of Hospital Care of Diabetic Patients: 2. A New Model for In patient Support Services. Clinical Diabetes. 2003; 21: 136-139.
Inpatient DM Management:Risks with Hyperglycemia Hyperglycemia is associated with increased in-hospital mortality, CHF, prolonged hospital stay, increased risk of infections1-4 Diabetes and hyperglycemia associated with poor outcomes in patients with CVA and CABG 1Capes, Lancet, 355: 773-778, 2000. 2 Umpierrez, J Clin Endo Metab, 87: 978-982, 2002. 3 Furnary, Circulation, 100: I-591, 1999. 4 Zerr, Ann Thorac Surg, 63: 356-361, 1997. 5 Capes et.al., Stroke, 32: 2426-2432, 2001. 6 Kiers et.al., J Neuro Neurosurg Psych, 55: 263-270, 1992. 7 Furnary, J Thorac Cardiovasc Surg, 125: 1007-1021, 2003
Inpatient DM Management:Glucose Control Makes a Difference Intensive IV insulin treatment after acute MI Intensive IV Insulin treatment in mechanically ventilated patients DIGAMI1 Van den Berghe2 Intensive insulin treatment improved longterm survival and risk reduction in mortality Dramatic risk reduction in ICU and overall in-hospital mortality 1 Malmberg, K. DIGAMI study group, BMJ, 1512-1515, 1997. 2 Van den Berghe, et.al., NEJM, 345: 1359-1367, 2001.
Intensive Insulin Therapy in The SICU : The First Leuven Study • 63% cardiac surgery • 8% thoracic surgery • 4% neurosurgery • 6% abdominal surgery • 4% vascular surgery • 4% trauma surgery • 4% transplant surgery Apache II score = 9 (7-13)
Blood Glucose Threshold in Cardiac Surgery and Critical Care • Lowest mortality occurs in patients with blood glucose levels < 150 mg/dL.Journal of Thoracic Cardiovascular Surgery 125: 1007-1029, 2003. • Anthony Furnary et al: Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Annals of Thoracic Surgery 67: 352-362, 1999.
Hyperglycemia as a Marker ofPoor Clinical Outcome • Non-ICU Setting: • Medicine-COPD, ESRD, ESLD • Infectious Diseases – Pneumonia • ICU/critical Setting • Acute Myocardial Infarction • Acute Stroke • General and Cardiovascular Surgery • ICU
Hyperglycemia and Acute Coronary Syndrome/MI • Diabetes is an independent risk factor for mortality in acute MI. • Mortality increased with blood glucose less than 70 and more than 120 mg/dL. • The higher the serum glucose, the greater the risk for mortality. • The strong association persisted after adjustment for multiple co-variables such as infarct size. • Patients without a history of diabetes were at greater risk.
Predictors of Poor Clinical Outcomes • Postoperative hyperglycemia • COPD Exacerbations with elevated hyperglycemia; the higher the glucose, the higher the mortality (> 167 mg/dL = mortality rate of 32%) • Trauma patients with hyperglycemia had increased morbidity and mortality
Intensive Insulin Therapy in the MICU:The Second Leuven Study • 42% respiratory failure • 25% liver failure • 8% heme-onc • 8% other sepsis • 4% cardiac • 4% neurology • 22% history of cancer • 20% renal failure • 22% received steroid Rx Apache II score = 23 (14-32) Increased hypoglycemia Less decrease in mortality -17.9%
META ANALYSES • Wiener, JAMA 2008 • 29 studies, N=8,432 • 1º - Hospital mortality (23.3% vs 21.6%) • Dialysis – no diff; • Septicemia – reduced with int control (surgical ICU setting). • Hypoglycemia RR 5.3 • Griesdale, CMAJ 2009 • 26 studies, N=13,567 • 1º - 90 daymortality (RR 0.93, I vs C) • Hypoglycemia RR 6.0 • ? Benefit for surgical pts
Insulin: Is it harmful or does it offer preischemic protection to the brain? • Harmful • Neuronal necrosis • Infarct or hemorrhage • Protective • Controls blood glucose, prevents focal ischemia • Interacts directly with the brain, prevents global ischemia
Preischemic Protection • Hyperglycemia aggravates ischemia in the spinal cord • A single small dose of insulin (0.5 units/Kg) prior to ischemia in rabbits was found to be protective. • There was no protection postischemia. Nagarni, D. et al. Anesthesia and Analgesia 2007; 105: 1397.
On-Pump CABG with Intraoperative IIT • IIT targeted to 80-100 mg/dl; conventional < 200 mg/dL • No reduction in perioperative morbidity and mortality • Statistically significant increase in the incidence of stroke in the IIT group and a trend toward increased mortality Gandhi, GY et al. Intensive intraoperative insulin therapy versus conventional glucose management during cardiac surgery: A Randomized trial. Annals of Internal Medicine 2007; 146: 233-43.
Aneurysmal Subarachnoid Hemorrhage Status after Surgical Clipping • IIT associated with decreased infection rate; 42 to 27% • No difference in incidence of • Vasospasm • Neurologic outcome • Mortality Bilotta F et al. The effect of intensive insulin therapy on infection rate, vasospasm, neurologic outcome, and mortality in Neurointensive care unit after intracranial aneurysm clipping in patients with acute subarachnoid hemorrhage: A randomized prosepective pilot trial. Journal of Neurosurgery Anesthesiology 2007; 19: 156-60.
Infrainguinal Vascular Surgery • Retrospective cohort study • Elevated glucose in postoperative phase is an independent risk factor for infection. • Vriesendorp, TM et al. Early post-operative glucose levels are an independent risk factor for infection after peripheral vascular surgery. A retrospective study. European Journal of Vascular and Endovascular Surgery 2004; 28: 520-525.
Organ Failure and Mortality • Hyperglycemia occurs early with median time to peak BG at 7 hours • Independently associated with organ failure and death Yung, M. et al. Pediatric Critical Care Medicine 2008, 9: 147.
Case Report-Preoperative Hypoglycemia • Type 2 insulin regimen recently changed from Novolog 70/30 Mix 30 units SQ AM and 20 units SQ PM to Detemir 55 units SQ in AM and Glulisine 5 Units SQ TID AC • Preoperative instructions: Take full dose of basal, no rapid-acting insulin • BG on arrival 68 mg/dL; took only 45 Units of Detemir • D5W initiated at 250 mL/hr, glucose 156 mg/dL • 3 hours later, glucose 47 mg/dL, surgery cancelled Preoperative Hypoglycemia in a Patient Receiving Insulin Detemir Olson, R, et al. Anesthesia and Analgesia. Vol. 108, 6, June, 2009
What was the problem? • “But if the dose is inappropriate, for example from a misguided attempt to provide both basal and bolus coverage with just basal insulin, the risk of hypoglycemia while fasting increases.” • Insulin dosing guidelines need to be followed.
What about glucose variability? • Standard deviations of BG significant predictor of ICU and in-hospital mortality among diabetic and nondiabetic patients • Stronger predictor than mean BG • Increased glycemic liability index but below average BG had almost 5-fold increase in odds of hospital mortality Ali N et al. Glucose variability is independently associate with mortality in patients with sepsis. Critical Care Medicine. 2007; 36: A 257. Monnier L et al. Activation of oxicative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA 2006; 295: 1681-7.
Current Standards/Guidelines • The Endocrine Society Clinical Practice Guideline Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting, 2012 • ADA/AACE Consensus Statement, June 2009 • Insulin therapy for persistent hyperglycemia; recommend threshold ≤ 180. • Goal 140-180 for most pts once insulin started. • Recommend using IV insulin. • Targeting glucose < 110 not recommended • Surviving Sepsis Campaign, 2008 • Intravenous insulin to control hyperglycemia in patients with severe sepsis. • Aim to keep blood glucose < 150.
Current Standards/Guidelines • Surgical Care Improvement Project • 0600 BG < 200 mg/dL POD # 1 and POD # 2 • 2014 Cardiac surgery patients with controlled postoperative blood glucose (less than or equal to 180mg/dL) in the timeframe of 18 to 24 hours after Anesthesia End Time. • Endocrine Society Statement, 2009 • Target blood glucose of 144-180 is reasonable, perhaps preferable, option in critically ill ICU patients. • American College of Surgeons • ACS has now requested the SCIP measure be removed citing need for more research, 2010 • 2012 Optimal Quality Care of Geriatric Surgical Patient • Society of Critical Care Medicine, 2012 • < 150 mg/dL; 110-140 mg/dL if low hypoglycemic rates • Anesthesia Patient Safety Foundation • < 200 mg/dL
Practice Recommendations Evidence based Expert opinion Clinical judgment
Hyperglycemia is Common in Surgical Patients • Inpatient Surgical Patients: UMMC • Hgb A1C elevated with no prior Dx of DM: 29% • Postop hyperglycemia in non-diabetic patients: 32%
Preoperative • A1C Value-Below 8% to schedule elective procedure • Optimize control • Cancel non-emergent at what value? • BG > 250, 300 • A1C > 9%
Preoperative • Insulin and Hypoglycemic Agents • Hold all short and rapid-acting insulins (prandial bolus) the morning of the procedure. • Give 80% of dose of long-acting insulin. • Give 66% of the usual morning dose of intermediate acting insulin. • Give 0 of mixed insulins to avoid the rapid component of these insulins. May need to order NPH for those on mixed insulins.
Preoperative • Insulin and Hypoglycemic Agents • Hold AM dose of oral hypoglycemic agents. • Hold incretin hormones day of surgery. • Insulin pump patients should continue their basal rate up until the time of surgery. Anesthesia will guide from there. • Take rapid-acting correction insulin as needed every 4 hours.
Preoperative • Inpatient • Insulin Pumps: Continue BASAL rate up until the time of surgery and NOTIFY ANESTHESIA for intraop management. Ideally a plan is in place prior to the procedure. • Insulin Drips: Continue BASAL rate up until the time of surgery and NOTIFY ANESTHESIA for intraop management
Preoperative • Nutrition • NPO • Sips of water to take some meds • TPN • If continued, consider dextrose source and the compound of the solution.
Hospital Pump Patient Assessment • Safety knowledge • Cognition • Dexterity • Visual Acuity • Pump operation • Self test of pump orders • Pump features and functions operational • Pump and insulin program • Accurate per physician orders • Insulin type correct in pump • Insertion site (describe)