Patellar Instability
Patellar Instability. Dr M Prud ’ homme-Foster PGY-4 December 8 th , 2011 Adpated from previous presentation by Dr. Ken Kontio. Talk Outline. Anatomy / Biomechanics (MPFL) Clinical presentation Physical examination Group demonstration Imaging Treatment Associated issues

Patellar Instability
E N D
Presentation Transcript
Patellar Instability Dr M Prud’homme-Foster PGY-4 December 8th, 2011 Adpated from previous presentation by Dr. Ken Kontio
Talk Outline • Anatomy / Biomechanics (MPFL) • Clinical presentation • Physical examination • Group demonstration • Imaging • Treatment • Associated issues • Lateral patellar tilt (aka. lateral facet syndrome)
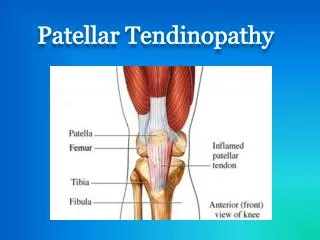
Anatomy • Medial structures most important • Importance of Medial Patello-Femoral Ligament recently noted • The anatomy and reconstruction of the medial patellofemoral ligament. Smirk C, Morris H. Knee. 2003 Sep;10(3):221-7. • Origin: posteromedial femoral epicondyle, just distal to adductor tubercle and post./inf. to this • Insertion: superomedial patella, undrsurface vastus medialis, quadricepts tendon
Biomechanics MPFL • Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. Conlan T, Garth WP Jr, Lemons JE. J Bone Joint Surg Am. 1993 May;75(5):682-93. • Biomechanical relative contribution to lateral translation studied • MPFL constributed 53% of total lateral restraining force (TLRF) • Other important medial stabilizers were the patellomeniscal ligament and the medial retinacular fibers, averaging 22% TLRF • Less important were the medial patellotibial band or transverse retinacular fibers • Speculated that these fibers may still hold importance in proprioceptive functions
Clinical Presentation • Subluxaton • History of “giving way” • As patella jumps from centralized position in trochlear grove • Lateral most common, (medial-iatrogenic?) • Commonly reduced by patient or spontaneously • Seldom objective xray or treatment ofdislocation • Occassionally traumatic start but most insidious onset • Often pre-existing conditions such as Genu valgum and ligament laxity • Associated swelling minor and symptoms retrictive for short duration
Clinical Presentaion Acute dislocation: • Direct • Direct blow to patella from ground or others • Often no predisposing factors • Indirect • Strong quadricepts contraction with flexed and valgus knee position, IR femur or ER tibia • Felt to dislocate over LFC in about 60-70 degrees of flexion Clinical: • Often immediate hemarthrosis • 40-50 percent, cartilage injury (LFC/MFP) • Reduction: • Relaxation • Medially directed force to unlock patella (spasm) • As knee extends, patella needs to come above LFC
Physical Exam • Need to carefully assess knee to rule out other causes of knee difficulty such as: • ACL, PCL, MCL tear • Can lead to instability sensations • Patello-femoral pain syndrome • Often co-exists with it but separate condition • More often chondromalacia patella exists also • RSD/RPS • Commonly involves knee area, disproportionate pain complaints
Physical Exam • General: • Ligament laxity (pes planus, hyperextension joints) • Specific: • Genu valgum (standing measurements) • Rotational Profile: Femoral antiversion (Prone measurements) • Patella Alta (not engaging by 15-20 degrees flexion) • Differentiate between functional versus anatomic type
Physical Exam • Wasted Vastus M. (thigh circumference) • Abductor strength • Increased Q-angle (sitting assessment-in flexion) • normal less 15 degrees men, less than 20 degrees females • Shallow lateral FG (try to assess trochlear depth) • Patellar shift (2/4 quadrants or less lateral translation)
P/E • Others • Apprehension sign (supine , 20° flex) • J-sign (pathonomonic- tight lateral structures) • Lateral subluxation when knee flexed -30° to full extension • Patellar translation (prone with relaxed quads) • Off end of bed holding affected leg • Bassett`s sign (ICL 1976) • Tenderness medial femoral epichodyle Boden et al. Patellofemoral Instability: Evaluation and Management. The Journal of the American Academy of Orthopaedic Surgeons (1997) vol. 5 (1) pp. 47-57
Radiologic Investigations • PA in 45° flexion and Lateral standard • Skyline view (axial) • Lauren 20 degrees, Merchant 40 degrees • Generally 30 degrees bend with beam directed 30 degrees caudad from femoral plane • Assesses patellar tilt and translation, congruence angle, Insall-Salvati index(LT:LP), sulcus • Will miss about 50 % osteochondral fractures • Especially fully cartilagenous fragments (not salvageable)
CT / MRI • CT occasionally used in assessment of chronic problems assessing patello-femoral relationship in different magnitudes of flexion • Documentation mainly, sensitive assessment-architecture • MRI • Acute scenario useful due to limited exam • Unlikely to change treatment unless bony fragment seen • Will confirm MPFL disruption if intervention planned • 100% effusion, 78% signal increase change and retraction VM, 87%bone bruise LFC, 30% bone bruise MPF (SO?)
Treatment (non-operative) General: • Strengthen out of pain range • 0-30 degrees flexion lowest PF contact pressures • Isotonic better than isometric • Closed chain better than open chain Acutely: • Aspiration to decrease inflammation, increase mobilization (fat globules?) • Lateral pad, short immobilization (1-2 weeks), patellar brace and ROM exercises • Strengthening, proprioception and sport specific training
Prognosis • Recurrence rate after first time: 15-44% • Recurrence rate for subsequent: 50% • 58% have limitation in strenuous activities @ 6months • Suggested that 55% fail to return to sports after dislocation Colvin and West. Patellar instability. J Bone Joint Surg Am (2008) vol. 90 (12) pp. 2751-62 Hawkins RJ, Bell RH, Anisette G. Acute patellar dislocations. The natural history. Am J Sports Med. 1986;14:117-20.
Study – Conservative Tx • Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. Atkin DM, Fithian DC, Marangi KS, Stone ML, Dobson BE, Mendelsohn C. Am J Sports Med. 2000 Jul-Aug;28(4):472-9. • 37 men, 37 women, avg. age 19.9yrs • 9% fmhx instability, 3% early childhood lower limb problems • 50% patella altaclincially • ROM 6 weeks 0-132 degrees, all returned before 6 mo, except kneel/squat • 6 mo58% difficulty with strenuous activity, otherwise normal population
Operative (Scope) • Acute • For osteochondral fractures visible • Unable to see MPFL (extra-articular structure) • Chronic • Consider superomedial portal to observe tracking • Look at patella for tilting / translation • Lateral facet aligns with trochlea 20-25 degrees flexion • Mid-patellar ridge aligns with trochlea 35-40 degrees flexion
Surgery-Reconstruction • Over 100 procedures described • Skeletally immature: • Need to consider non-osseous procedures • Generally fall into: • Proximal realignment (VM advancements, med. Imbrication) • Tendon transfer ( Galeazzi procedure) • ST transfer to medial patella • Patellar ligament transfer (Roux-Goldthwait) • Lateral half patellar ligament transferred to medial side
Study • Recurrent dislocation of the patella treated by the modified Roux-Goldthwait procedure. A prospective study of forty-seven knees. Fondren FB, Goldner JL, Bassett FH 3rd. J Bone Joint Surg Am. 1985 Sep;67(7):993-1005. • 37 pts, 47 knees, 10 males, 27 females • Modified Roux-Goldthwait • (LRR, medial transfer PL without advancement, MR plication, VM advancement) • F/U 5.8 yrs, E-12, G-31, F-1, P-3 (CMP)
Study • Semitendinosus tenodesis for repair of recurrent dislocation of the patella in children. Letts RM, Davidson D, Beaule P. J Pediatr Orthop. 1999 Nov-Dec;19(6):742-7. • 22 children, 26 knees, avg. age 14+4yrs, F/U 3+2yrs • All more than 3 dislocations • 17/26 had pre-existing CMP symptoms • At F/U 88% asymptomatic, 12% PF symptoms, all stable
Study • Reconstruction of the medial patellofemoral ligament for the treatment of habitual or recurrent dislocation of the patella in children. Deie M, Ochi M, Sumen Y, Yasumoto M, Kobayashi K, Kimura H. J Bone Joint Surg Br. 2003 Aug;85(6):887-90. • Galeazzi procedure • Corrected tilt angle and lateral shift ratio • Not able to fully correct hypermobility or patella alta
Surgery-Reconstruction • Skeletally Mature: • Options include ST procedures but generally not as successful especially in ligamentously lax individuals • General consensus is distal bone procedure • Often main deformity (Q-angle >15-20 degrees) • consider angular realignments if needed (sever genu valgum, Femoral antiversion) • Aim is to realign pull of quadricepts • Concern is patellofemoral contact pressures
Classic • Hauser procedure • Direct medial transfer tibial tubercle • Posteriorization due to tibial slope increased PF contact forces • Fulkerson (Clinical Orthopedics-1984) • Fulkerson et al. (AJSM -1990) • Antero-medial transfer tibial tubercle • Modification of distalization of functional patella alta
Study • Acta Orthop Traumatol Turc. 2007;41(1):21-30. Links [Fulkerson osteotomy for the treatment of chronic patellofemoral malalignment.] [Article in Turkish]Karamehmetoğlu M, Oztürkmen Y, Azboy I, Caniklioğlu M. • 21 knees, 18 pts, 10F, 8 M, avg. age 28.6 years • All had Outerbridge 111-1V level patellofoemoral degenerative changes • Anteriorization 10.5 mm average, VM advancement 7 knees • E/VG/G- 87%, F-9.5%, P-4.8%
Recent Interest – MPFL recon. • Results of medial patellofemoral ligament reconstruction in the treatment of patellar dislocation. Drez D Jr, Edwards TB, Williams CS. Arthroscopy. 2001 Mar;17(3):298-306. • Prospective case series, (19 patients), 15 F/U 31 mo • Autogenous Gracilis and /or semitendinosis, strip facia lata • G/E 13 (93%), F/P 2 (7%) • All attained previous activity levels
Study – MPFL reconstruction • Arthroscopy: The Journal of Arthroscopic & Related SurgeryVolume 20, Issue 2, February 2004, Pages 147-151 Medial patellofemoral ligament reconstruction with semitendinosus autograft for chronic patellar instability: a follow-up study Joäo Luiz Ellera Gomes M.D.,Ph.D., Luiz Roberto Stigler Marczyk M.D., M.Sc., Paulo César de César M.D. and Carlos Francisco Jungblut M.D. • 16 knees, Q>20 degrees or >10 degrees valgus – excluded • 5 yrs F/U • E-11, G-3, F/P-2 • Crepitus 10 knees post op
MPFL Reconstruction • Technical Errors During Medial Patellofemoral Ligament Reconstruction Could Overload Medial Patellofemoral Cartilage A Computational Analysis John J. Elias, PhD*, and Andrew J. Cosgarea, MD The American Journal of Sports Medicine 34:1478-1485 (2006) • Cadaver study • Looked at positioning and tensioning of autograft reconstruction • >5 mm proximal and >3 mm shortening led to 50% increase in the medial patellofemoral contact pressures
Other • Patellar tilt • Often cited for cause of patellar pain • Need tightness lateral retinaculum, some translation but primarily convergence (lateral) angles • Only TRUE indication for isolated retinacular release • CAUTION: • Seldom if ever is lateral release indicated as a sole procedure in patellar instability (often worsens situation)
Other Good References • Journal of Bone and Joint Surgery - British Volume, (2007) Vol 89-B, Issue 6, 709-716. Assessment and management of chronic patellofemoral instability J. S. Mulford, FRACS, Senior Knee Fellow1; C. J. Wakeley, FRCR, Consultant Radiologist; and J. D. J. Eldridge, FRCS, Consultant Orthopaedic Surgeon • JAAOS 1997, 5(1) 47-57 Patellofemoral Instability : Evaluation and Management Boden BP, Pearsall AW, Garrett WE Jr, Feagin JA Jr.