Chronic Obstructive Pulmonary Disease (COPD)
Chronic Obstructive Pulmonary Disease (COPD). Angela Voraotsady. Definition Epidemiology Clinical Aspects Treatment Effects of Exercise Exercise Testing Exercise Prescription Summary and Conclusion References. Outline . Chronic: It’s long-term and doesn’t go away Obstructive:

Chronic Obstructive Pulmonary Disease (COPD)
E N D
Presentation Transcript
Chronic Obstructive Pulmonary Disease (COPD) Angela Voraotsady
Definition • Epidemiology • Clinical Aspects • Treatment • Effects of Exercise • Exercise Testing • Exercise Prescription • Summary and Conclusion • References Outline
Chronic: It’s long-term and doesn’t go away • Obstructive: The flow of air from the lungs is limited • Pulmonary: Another word for lungs and breathing • Disease: It’s a health problem that needs to be taken seriously Chronic Obstructive Pulmonary Disorder
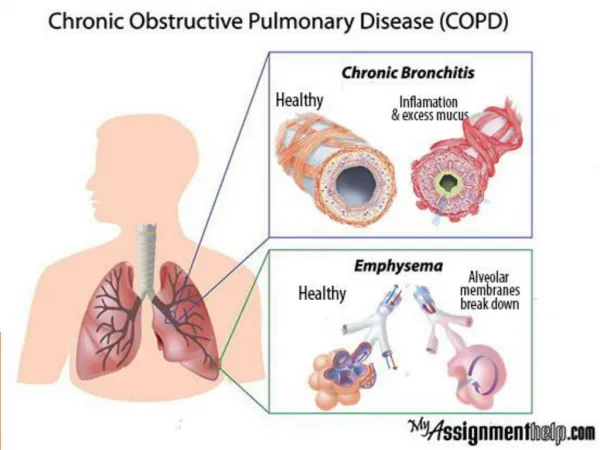
A progressive condition that includes chronic bronchitis or emphysema or both. • Smoking is the primary cause of COPD. • 80% of the people affected by COPD are current or former smokers. • Other risk factors are: occupational and environmental pollutants, alpha antitrypsin deficiency, allergies and asthma, poor nutrition, periodontal disease and low birth weight. What is COPD and what causes it
Chronic Bronchitis Emphysema The tiny air sacs get over-stretched and break down. When this happens old air gets trapped inside and new air cannot get in. • Airflow is limited by narrowed airways. The narrowed airways are caused when damaged airways get tight, swollen, and filled with mucus. So what does that mean?
COPD is the most prevalent chronic pulmonary disease and affects an estimated 24 million Americans. • COPD is the fourth most common cause of death in the United States and is the only cause in the top ten that continues to rise. • COPD accounts for approximately 100,000 deaths each year. • By 2020, it is estimated to be the third leading cause of death in the United States and the fifth leading cause of disability in the world. • It is most commonly found in white males over the age of 60. Epidemiology
Symptoms • Cough that produces mucus, may be blood streaked • Shortness of breath aggravated by exertion or mild activity • Wheezing • Rales (small clicking, bubbling, or rattling sounds in the lung) • Fatigue • Ankle, feet and leg edema that affects both sides • Reddish cheeks • Reddish face, palms, or mucous membranes (such as the inside of the mouth) • Headaches • Vision abnormalities Clinical Aspects
Spirometry is the best way to test for COPD. It is simple and can be interpreted immediately. Listening to the lungs with a stethoscope can sometimes work too but sometimes the lungs sound normal even when COPD is present. X-rays and CT scans can also be performed; but these can also look normal even if COPD is present. Sometimes a blood test called a “blood gas” is required to measure the amounts of oxygen and carbon dioxide in the blood. Laboratory Diagnosis
Medical • Bronchodilators are prescribed to open the airways • Inhaled steroids to reduce lung inflammation. • In severe cases or during flare-ups steroids may be needed intravenously or by mouth. • Antibiotics can also be prescribed when a patient has an infection prevent COPD from becoming worse. • Oxygen therapy may also be needed at home if the patient has low oxygen levels in their blood. Treatment
Surgical • Removal of parts of diseased lung in patients with emphysema. • Lung transplants may be required in severe cases Treatments
Hyperinflation resulting from impeded exhalation, incomplete lung emptying, and air trapping. Static hyperinflation can be caused from daily living and when exercise occurs dynamic hyperinflation can be superimposed on static hyperinflation. Dynamic hyperinflation is related to increased breathing frequency and affects the mechanical efficiency of ventilation leading to breathlessness. Effects on Ability to Exercise
In patients with emphysema there is a impairment of gas exchange due to the destruction of the alveolar-capillary membrane. Breathing efficiency is thus worsened by an increase in VD/VT and can also cause hypoxemia during exercise. • Chronic hypoxemia can also cause erythrocytosis which can further complicate circulation during exercise. • Smokers will have an increase in carboxyhemoglobin, impairing the blood oxygen transport system. • Other symptoms of COPD can also affect different individuals personally. Effects on Ability to Exercise
Beta2-adrenoceptor (sympathomimetic) agonist reduce peripheral vascular resistance and can cause tachycardia, palpitations and tremulousness. • Methylxanthines can cause tachycardia, cardiac dysrhythmias, and CNS stimulation with increased respiratory drive and a risk of seizures. • Thiazide diuretics and loop diuretics can cause hypokalemia that can in turn cause cardiac dysrhythmias and muscle weakness • Glucocorticoids(prednisone) can cause skin atrophy and fragility, osteoporosis, muscle atrophy, and myopathy. • Antidepressants cause resting and exercise tachycardia. • COPD often coexists with cardiovascular diseases so the effects of medications taken for cardiovascular disease needs to be reviewed as well. Effects of Medication on Exercise
Acute effects Chronic effects Cardiovascular reconditioning Reduced ventilatory requirement at a given work rate Improved ventilatory efficiency Reduced hyperinflation Desensitization to dyspnea Increased muscle strength Improved flexibility Improved body composition Better balance Enhanced body image • Increased verbal processing • Dynamic hyperinflation – further reduces inspiratory capacity and smaller tidal volume Effects of Exercise
Maximal testing is safe with appropriate monitoring. • The cycle ergometer is best for controlling external work rate, measuring gas exchange and blood sampling. • But patients might be more willing to perform treadmill testing. • During testing a near-linear increase in work rate should be attempted with incremental adjustments being made to speed and grade. • The goal is to be able to get between 8-12 minutes of exercise data. Exercise Testing
The Bruce Protocol Equipment required: treadmill, stopwatch, pencil, paper for recording Procedure: The treadmill is started at 1.7 mph and at an incline of 10%. At three minute intervals the incline of the treadmill increases by 2% and the speed increases as in the table to follow. Exercise Testing
Exercise rehabilitation should include several different professionals including respiratory therapists, physical therapists and exercise professionals, and occupational therapists. • Respiratory therapists will evaluate, teach, and ensure effective use of bronchodilator medications and oxygen therapy. • Physical therapists and exercise professionals will evaluate exercise endurance, muscle strength, flexibility and body composition along with monitoring the exercise prescription and monitoring exercise performance. • Occupational therapists will evaluate activities of daily living and quality of life so they are able to teach energy conservation and body mechanics aimed at reducing the oxygen requirement for specific activities • All therapists will teach improved breathing efficiency with methods such as pursed lips and diaphragm breathing. Exercise Prescription
Pursed lips method Diaphragm breathing Put one hand on your upper chest, and the other on your belly just above your waist Breathe in slowly through your nose - you should be able to feel the hand on your belly moving out. The hand on your chest shouldn't move. Breathe out slowly through your pursed lips - you should be able to feel the hand on your belly moving in as you exhale (breathe out). • Breathe in slowly through your nose for 1 count • Purse your lips as if you were going to whistle • Breathe out gently through pursed lips for 2 slow counts (breathe out twice as escape naturally- don't force the air out of your lungs • Keep doing pursed lip breathing until you're no longer short of breath Exercise Prescription
Modes of exercise can be walking, cycling, swimming, or conditioning exercises such as tai chi. The mode should be enjoyable to the patient and directly improve ability to perform usual daily activities. • For patients with oxyhemoglobin desaturation of less than 88% or a documented reduction in arterial oxygen tension of less than 55 mmHg oxygen should be administered during exercise. The goal for oxygen therapy is to maintain oxyhemoglobin saturation above 90%. Exercise Prescription
Aerobic – large muscle activities • 1-2 sessions, 3-5 days/week • 30 min/sessions with an emphases of duration rather than intensity • Strength – free weights, isokinetic/isotonic machines • Low resistance, high reps 2-3 days/week • Flexibility – stretching, tai chi • 3 days/week • Neuromuscular – walking, balance exercises, breathing exercises Exercise Prescription
Often patients with COPD cannot perform 20-30 min of exercise so 5 or 10 min intervals of exercise may be necessary in the beginning. • Group interaction is helpful in the reconditioning process since an individual with COPD is at a particular risk of relapsing into a state of inactivity and physical deconditioning. Exercise Prescription
COPD is a major killer in the world. • It cannot be controlled but quality of life can be enhanced through medications and lifestyle changes. • Exercise training is a crucial aspect of clinical management and the rehabilitation of individuals suffering from COPD. Summary
Cooper, C. B. (2001). Exercise in chronic pulmonary disease: limitations and rehabilitation. Medicine & Science in Sports & Exercise, 33(7), S643-S646. • Durstine, J. L., Moore, G. E., Painter, P. L., & Roberts, S. O. (2009). ACSM's Exercise management for Persons With Chronic Diseases and Disabilities (3 ed.). Champaign, IL: Human Kinetics. • Emery, C. F., Honn, V. J., Frid, D. J., Lebowitz, K. R., & Diaz, P. T. (2001). Acute Effects of Exercise on Cognition in Patients with Chronic Obstructive Pulmonary Disease . American Journal of Respiratory and Critical Care Medicine, 164, 1624-1627. Retrieved February 14, 2011, from http://ajrccm.atsjournals.org/cgi/content/full/164/9/1624 • Expert's Guide to Better Breathing. (2006). USA: BoehringerIngelheim Pharmaceuticals. • McArdle, W. D., Katch, F. I., & Katch, V. L. (2006). Optimizing Body Composition, Successful Aging, and Health-Related Exercise Benefits. Essentials of Exercise Physiology (3 ed., pp. 665-704). Philiadelphia, PA: Lippincott Williams &Willkins. • PubMed Health - Chronic obstructive pulmonary disease. (n.d.). National Center for Biotechnology Information. Retrieved February 16, 2011, from http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001153 • APA formatting by BibMe.org. References