Download
1 / 68
700 likes | 964 Vues
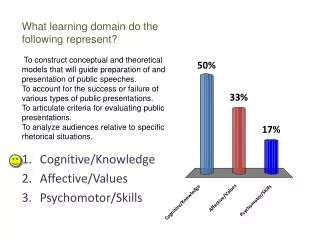
PSYCHOMOTOR SKILLS IN RESIDENCY TRAINING. Jose Y. Cueto Jr., MD, MHPEd Chairman, 2012 Professional Regulatory Board of Medicine Professional Regulation Commission. Objectives for the session:. 1. Discuss the educational principles behind the acquisition and development of psychomotor skills

E N D
PSYCHOMOTOR SKILLS IN RESIDENCY TRAINING Jose Y. Cueto Jr., MD, MHPEd Chairman, 2012 Professional Regulatory Board of Medicine Professional Regulation Commission
Objectives for the session: 1. Discuss the educational principles behind the acquisition and development of psychomotor skills 2. Examine required number of operations for OB-GYN residents 3. Discuss research studies relevant to training and how to utilize research data 4. Formulate a system of determining and validating requirements in number of operations in residency training (both for graduation and for certification) 5. Formulate a system of documentation and reporting
Objectives for the session: 6. Determine how the number of operations performed during residency will affect credentialing and privileging in hospitals 7. Discuss performance-based evaluation, specifically the Objective Structured Clinical Exam (OSCE)
Main Objective of Training NOVICE COMPETENT EXPERT SURGEON
I. Educational Principles • Fitt and Posner (1967): 3 phases of skills acquisition • Miller’s Pyramid
Fitt and Posner: 3 Phases 1. Cognitive phase 2. Associative phase 3. Autonomous or Fixation phase
Progression of Skills Acquisition and Development 2nd Assist (mainly exposure) 1st Assist (limited participation in procedure) Surgeon (under direct supervision) Surgeon (independently performing)
My Observation • Description of The Residency Training Programs should include a section on Psychomotor Skills • Include an explanation on the required number of operations using statistics • Clarify the progression of operative cases handled by residents and provide the basis • Documentation and reporting found in “Basic Requirements for Examination”, page 42; but not discussed in the curriculum (same requirements for graduation and certification)
General Principles • Progression: Trainees first learn simple tasks, before they progress to procedures of medium difficulty, and finally to complicated procedures • Transfer of learning / transfer of skills: what trainees learn from simple skills are utilized in the performance of medium and complicated skills • Trainees need to learn to pay attention to details, follow proper sequence, observe meticulous technique
Application of Principles 1. The simpler the procedure, the shorter it takes to learn, and the less number of cases needed to master it 2. The more complicated the procedure, the longer it takes to learn, and the more number of cases needed to master it 3. The more complicated the procedure, the higher the need for supervision and guidance
Implementation Residency Training Committee 1st yr 1st yr 2nd yr 3rd yr 4th yr
III. Researches 1.Does Residency Training Improve Cognitive Competence in Obstetric and Gynaecologic Surgery?, Balayla, Abenhaim and Martin, McGill University, Montreal, Can, J ObstetGynaecol Can 2012;34(2):190–196 2. Competency-based Residency Training: The Next Advance in Graduate Medical Education, Donlin Long, MD, PhD, Johns Hopkins University School ofMedicine, Academic Medicine, Dec 2000
Researches 3. Factors Associated with a Successful Outcome in the PBS Certifying Examinations, Crisostomo and Marfori, Philippine Journal of Surgical Specialties, Oct-Dec, 2010
Does Residency Training Improve Cognitive Competence in Obstetric and Gynaecologic Surgery? (JOGC,2012) Objectives: 1.To develop an operative knowledge assessment tool to evaluate thecognitive competence of trainees in obstetric and gynaecologic surgery 2.To determine the rate of change in competence during a five-year residency program .
J Obstet Gynaecol Can Methods: • Twenty-eight participants in five training groups (PGY-1 to PGY-5) in McGill University’s residency program in obstetrics and gynaecology • Evaluation based on surgical cognitive competence (SCC) assessment tools • Three different obstetric and gynaecologic operations: open total abdominal hysterectomy (TAH), Caesarean section, and laparoscopic bilateral tubal sterilization (BTL)
J Obstet Gynaecol Can Performance of an operation/procedure Three fundamental components: 1. cognitive factor 2.technical element 3. judgment component
J Obstet Gynaecol Can Summary of Findings:
J Obstet Gynaecol Can Findings: • At level of PGY-5, residents had 100% surgical cognitive competence • This type of information may be helpful in ascertaining howlong a residency program should be
Competency-based Residency Training: The Next Advance in Graduate Medical Education (AM, 2000) • Donlin Long, MD, PhD • Professor of Neurosurgery, Johns Hopkins University • Studied NSS residents • Introduced competency-based program
Academic Medicine Traditional Program Competency-based Program 1. Fixed number of years 2. Residents have to learn all specified knowledge and skills in the allotted time 3. Problem of evaluating competence of every resident 4. Graduate may not be competent to perform required procedure or manage particular patients. 1. Specifies maximum duration 2. Time taken to acquire knowledge and skills is based on the abilities of individual trainees 3. Evaluation of every resident in every procedure 4. Resident is evaluated and certified to have acquired competence and confidence to practice independently
Factors Associated with a Successful Outcome in the PBS Certifying Examinations (PJSS, 2010) Objective: To determine the factors associated with a successful outcome in the PBS certifying exams (written and oral) Method: Retrospective, cross-sectional study utilizing 370 candidates from 2006-2009, with 137 (37.0%) successful outcomes
PJSS Significant Factors: • Younger age of examinees • Previous performance in the RITE • Taking the exam within a year of completion of residency • Training in a university-based program • Undertaking subspecialty fellowship during the examination year
PJSS Other Factors (Not Significant) • Sex (M-F) • Marital Status • Case volume • Continuous/interrupted program • Location of training program (MM vs. outside)
PJSS CASE VOLUME performed during residency (major operative procedures): 1. High volume: 299 0r more cases (upper 3rd) 2. Medium volume: 171-298 cases (middle 3rd) 3. Low volume: less than 171 cases (lower 3rd) NOTE: did NOT influence performance in written and oral exams
Open for further research • Relationship of case volume to: 1. surgical cognitive competence 2. technical element 3. judgment component
The essential messages 1. The process of acquiring and developing operative skills is more important than the output (number of operations performed). 2. Quality is more important than quantity. 3. Supervision and feedback are critical. There may be institutions where residents get to perform so many operations by themselves, but they never get to know which steps are done correctly or incorrectly.
The Essential Messages 4. The cognitive factor and the judgment component are very critical in the performance of procedures 5. The fixed duration of residency training may not be appropriate for a number of residents
Determining Requirements Factors to consider: 1. Degree of difficulty: simplicity / complexity of procedure /low-risk / high-risk *The simpler the procedure, the lower the number required to acquire competence *The more complex / complicated the procedure, the higher the number required to acquire competence
Determining Requirements Factors to consider: 2. Trainee factor: fast / slow learner dexterity with procedures *The fast learner and the trainee with dexterity / adeptness at performing procedures will require lower number of cases *The slow learner and the trainee with “clumsiness” in performing procedures will need a higher number of cases
Determining Requirements Factors to consider: 3. Institutional factor: high volume vs. low volume private vs. charity/service patients *The resident belonging to a high-volume hospital will require a lower number of cases (reinforcement) *The resident belonging to a low-volume hospital will require a higher number of cases (too few and far in-between)
Determining required number of operations 1. Use of the Delphi technique • 12-30 Experts • List of operations • 3 rounds • Questions to answer
Questions Based on your experience and expert opinion: • How many times should a resident assist in the following procedure before he can be given his first case? • How many times should a resident perform this procedure under direct supervision before he is allowed to perform it independently? • How many times should a resident perform this procedure before he can acquire the competence and the confidence to perform it safely on his own?
Three Rounds Round 1: 12-30 experts give their proposed number of operations, based on the questions; without them communicating with each other Round 2: the experts are given feedback on how their colleagues answered the questions (tabulation of results); afterwards they are asked for their modified list of proposed number of operations Round 3: the experts are gathered and they are asked to arrive at a consensus regarding required number of operations
Validation Stage 1. Identify institutions: • Government • University-based • Private 2. Conduct a parallel research study: longitudinal tracking of residents until they get to the certifying exams 3. Based on results, modify/maintain the requirements
My Observation • Notation: Starting 2006, only 70% of cases with complete transfer of technical responsibility is allowed • What is the basis for the policy? • What problem does it solve? Lack of residents’ cases? • Consultants’ cases given to residents: fall under 2nd column (supervised cases) • Private cases: no complete transfer of responsibility demo cases to show residents how procedures should be done
Residents’ Responsibilities 1. provide preoperative evaluation, assessment of risks 2.identify indications/contraindications to planned procedure, possible complications 3. perform the procedure, modifying it in presence of unforeseen conditions 4. providing immediate and long-term care. Note: For private patients, decisions will always be made by the Attending Consultant (The judgment component is lacking)