Download
1 / 137
1.4k likes | 1.99k Vues
Podiatry essentials the basic foot exam. Amy Splitter, DPM ACMC Division Chief, Division of Podiatry Assistant Professor, California School of Podiatric Medicine at Samuel Merritt University. Introduction. Four Basic Elements to lower extremity foot exam Vascular Neurological

E N D
Podiatry essentials the basic foot exam Amy Splitter, DPM ACMC Division Chief, Division of Podiatry Assistant Professor, California School of Podiatric Medicine at Samuel Merritt University
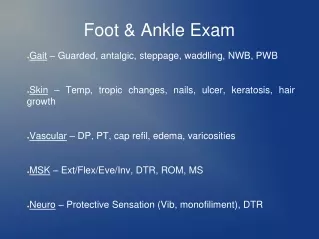
Introduction • Four Basic Elements to lower extremity foot exam • Vascular • Neurological • Dermatological • Musculoskeletal
The vascular history • How far can you walk? • Major Risk Factors • Tobacco • Diabetes mellitus • HTN • Cardiac disease • CVA • Family history
Vascular evaluation: inspection • Skin color, temp • Skin thickness and texture • Digital hair • Toenail condition
Pedal Pulses • Dorsalispedis (DP) • Posterior tibial (PT) • Perforating peroneal (PP)
Dorsalis pedis pulse Palpate here EHL Tendon
Posterior tibial pulse Medial malleolus Palpate here
Quantifying pedal pulses Absent, Diminished, Palpable, Bounding vs. 1+, 2+, 3+, 4+
Capillary Refill (SPVPFT) • The time it takes to completely fill the area of pallor • Normal: < 3 seconds • PAD: > 10 sec
Capillary refill technique 1. Place foot at heart level
Capillary refill technique 2. Squeeze blood from the hallux
Capillary refill technique 3. Observe time for blood return
Capillary Refill (SPVPFT) Common Errors • Digit below heart level • Residual venous blood
Doppler technique Apply acoustic gel
Doppler Sounds Normal PT Abnormal DP Normal hallux artery Vein
ABI Interpretation • Ankle pressure/Brachial pressure • Normal 1.0 – 1.2 • Grossly abnormal <0.5
ABI Pitfalls • Does not measure collateral flow • Cannot confirm flow distal to probe • Interpret results in diabetics with caution
Common LE neurological problems • DM neuropathy • IM neuroma • Tarsal tunnel syndrome • Nerve impingement • CVA
Neurological workup • PMH, ROS: Any potential causes of neuropathy? • Diabetes mellitus • Prior surgery • Nerve injury • Medications • Lower back problems • CVA
Neurological workup • Personal History: Any potential causes of neuropathy? • EtOH abuse • Occupational exposures • Chemotherapy • HIV • Elderly • Many different causes
Where’s the neurological problem? • Local • Regional • Sensory • Autonomic • Motor-UMN vs. LMN
UMN vs. LMN Upper Motor Neuron • Affects groups of muscles • Only slight atrophy • Spasticity with hyperreflexia • No fasiculations • Normal nerve conduction studies Lower Motor Neuron • Affects individual muscles • Atrophy • Flaccidity, hypotonia and hyporeflexia • Fasiculations • Abnormal nerve conduction studies
Neurological Physical Exam • Sensory examination • Motor examination • Sensory-motor examination • Gait
Neuropathy Workup: Physical Exam • Compare right to left • Compare distal to proximal • Nerve injuries can be subtle
Sensory Examination • Depends on the subjective response of the patient • Focus your testing based on the HPI
Sensory Examination: Instruments • Safety pin • Semmes-Weinstein 10 gm monofilament • Q-tip • 128 Hz tuning fork • Paper clip
Sensory Examination • Vibratory • Proprioception • Pain • Temperature • Pressure (protective sensation) • 2 point discrimination • Light touch • Percussion
Sensory Examination • For each sensory test, you should consider the following: • Which nerve is being tested? • Which dermatome is being tested? • What spinal pathway is being used?
Sensory Testing: Semmes-Weinstein Monofilament • Tests pressure sensation • Uses: • R/o LOPS • Map out sensory deficit
Sensory Testing: Semmes-Weinstein Monofilament • Prerequisites • Patient understanding • Non-callused skin
Sensory Testing: Semmes-Weinstein Monofilament • Prerequisites • Patient understanding • Non-callused skin
Sensory Testing: Semmes-Weinstein Monofilament Demonstrate that this won’t hurt
Sensory Testing: Semmes-Weinstein Monofilament Show the patient what to expect
Sensory Testing: Semmes-Weinstein Monofilament Start distally
Sensory Testing: Semmes-Weinstein Monofilament Bend the filament, then release