Download
1 / 74
740 likes | 1.03k Vues
Elbow, Forearm, Hand and Wrist. Terminology. Epicondyle: A bony protuberance above a condyle that serves as an attachment point for muscles, ligaments or tendons. Terminology.

E N D
Terminology • Epicondyle: A bony protuberance above a condyle that serves as an attachment point for muscles, ligaments or tendons.
Terminology • Extensor/Suppinator: a group of muscles located on the posterior surface of the forearm that produce the combined motions of wrist extension and wrist suppination. • Flexor/Pronator: a group of muscles located on the anterior surface of the forearm that produce the combined motions of wrist flexion and wrist pronation.
Terminology • Hyperextension: a force that causes a joint to extend beyond normal anatomical limits. • Tinel’s sign: ulnar nerve paresthesia that results when the ulnar nerve is tapped by the examiner near the elbow. A positive Tinel’s sign is an indication of ulnar nerve involvement/impairment. • Valgus: a force that bends a joint to the side in an inward direction. Also referred to as abduction force mechanism. • Varus: a force that bends a joint to the side in an outward direction. Also known as adduction force mechanism
Terminology Genetic Hypermobility: a condition in which an individuals joints can move beyond normal anatomical limits. Intracondylar: the area of a bone that is between two condyles, usually at the distal end of a bone that forms a hinge joint. Supracondylar: the area of a bone that is directly above the condyles, so just proximal to the joint.
Terminology • Epicondylitis-Swelling and irritation of an epicondyle at the point where muscle originates • Little League Elbow-Medial elbow epicondylitis • Tennis Elbow-Lateral elbow epicondylitis • Traction Apophysitis-Swellingand irritation at the apophyseal area of immature bone due to repetitive traction force
Terminology • Criteria-The measurable standards an injured athlete must demonstrate in order to progress from one phase of rehab to the next • Therapeutic—Healing action • Phase I—Time immediately following injury or surgery which movement in affected part is limited to ease pain; pain management
Terminology • Phase V - Time when the athlete begins to re-develop sport-specific skills by performing exercises that mimic movement specific to the injured athletes sport • Phase VI - The last phase of rehab when the athlete is gradually allowed to return to full practice and competition
Terminology • Phase II—Time when more vigorous therapeutic action initiated including joint range-of-motion, mobility and flexibility exercises • Phase III - Timein the rehabilitation process when strengthening exercises are introduced in an attempt to reverse the affects of atrophy from disuse during Phases I and II • Phase IV - Time in the rehab process when the athlete has re-developed basic strength and begins to work on speed, power and endurance
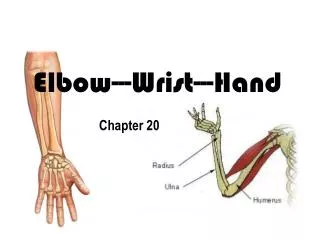
Skeletal Anatomy • Humerus • Lateral Epicondyle • Medial Epicondyle • Radius • Head • Neck • Ulna • Olecranon
Elbow Skeletal Anatomy Olecranon Fossa Humerus Humerus Coronoid Fossa Olecranon Process Capitulum Trochlea Lateral Epicondyle Medial Epicondyle Lateral Epicondyle Radial Head Ulna Ulna Radius Radius Neck of Radius
Joint Classification: Movement Joints Joint Name Radial-Humeral Ulnar-Humeral Radial-Ulnar Hinge: Flexion/Extension Hinge: Flexion/Extension Pivot: Rotation (Pronation/Suppination)
Elbow Motions • Flexion • Extension • Pronation • Suppination
Muscles that move the forearm Muscle Origin/Insertion Action Biceps Brachii Scapula/Radius Triceps Brachii Scapula/Ulna Brachialis Humerus/Ulna BrachioradialisHumerus/Radius Elbow Flexion (PM) Elbow Extension (PM) Elbow Flexion (S) Elbow Flexion with forearm suppinated
Muscles that move the Wrist Muscles Origin/Insertion Action Ext/Supp Lateral epicondyle/Ulna Flex/Pro Medial epicondyle/Radius Extension/Suppination Flexion/Pronation
Muscles that move the Fingers Muscles Origin/Insertion Actions Extensors Radius & Ulna/Phalangies Flexors Radius & Ulna/Phalangies Finger Extension Finger Flexion
Elbow/Forearm Strains • Bicep/Tricep strains are common, especially during auxiliary training periods such as weight training • Forearm strains are less common but also occur during weight training activities
Elbow/Forearm Strain • MOI: • Excessive force applied to musculature in an effort to overcome excessive resistance • Excessive repetition of an exercise movement • Inadequate recovery period between exercise sessions • S/S: • Pain and soreness in muscle belly and/or associated tendon • Possible swelling, Loss of function
Elbow Forearm Strain • Tx: • RICE • Cessation of offending activity • Stretching of affected musculature
Elbow Sprains • Common contact and throwing sport injury • Ulnar Collateral Ligament (UCL) most commonly involved • MOI: • Valgus force • Hyperextension force • Improper throwing mechanics leading to excessive and repetitive valgus force
Elbow Strains • S/S: • Pain/Point tenderness over ulnar collateral ligament • Positive valgus force stress sign (pain, joint laxity) • Swelling • Possible positive Tinel’s sign • TX: • RICE • Mild stretching/ROM exercises • Thermotherapy after initial 48-72 hours post-injury • Gradual strengthening exercises
Elbow Fracture • Epiphyseal and/or avulsion fractures of the medial epicondyle or the olecranon process are most common in adolescents • Supracondylar fractures of the humerus are not common but occasionally occur in contact sports • Intercondylar fractures of the humerus are rare • Other fractures associated with the elbow include the proximal radius and ulna
Elbow Fractures • MOI: • Powerful muscular contraction applied to the medial epicondyle or the olecranon process (avulsion fracture) • Powerful valgus or varus force with the elbow locked in a fully extended position (supracondylar fracture) • Extreme hyperextension force (supracondylar fracture) • Direct impact (intracondylar fracture)
Elbow Fracture • S/S: • Point tenderness over the medial epicondyle or olecranon process in cases of epiphyseal or avulsion fracture • Obvious deformity (especially present with supracondylar fractures) • Pain 2 inches above the elbow joint on the medial aspect (high suspicion for intercondylar fracture) • Tx: • Refer to ER • RICE, Splint
Forearm Fracture • Very common in youth sports injury • Often involves both the radius and ulna • When both-bone forearm fractures are located at the distal forearm near the wrist they are termed Colles’ fractures • MOI: • Fall on the outstretched hand (Colles’ Fracture) • Fall on the back of the outstretched hand (Reverse Colles’ Fracture) • Direct Blow
Forearm Fracture • S/S: • Athlete reports feeling a “pop” or “snap” • Obvious Deformity (false joint) • Pain, Swelling, Crepitus • TX: • RICE, Splint, Sling • MD Referral
Elbow Dislocation • Ulna is dislodged from the humerus • Most often ulna moves posteriorly • Somewhat common injury, especially in contact/collision sports • MOI: • Violent hyperextension force • Severe blow to the lateral aspect of the elbow while weight is being supported on the hand • Genetic Hypermobility
Elbow Dislocations • S/S: • Obvious Deformity • Severe Pain, Loss of Function • Tx: • Treat as a medical emergency • Splint arm/elbow in the position it is found in • Check distal pulses and sensation for vascular and/or nerve impairment
Elbow Bursitis • MOI: • Overuse • Chronic irritation • Bursa can also be ruptured by a direct blow • S/S: • Swelling, inflammation deformity • Pain, point tenderness over a bursa • Loss of joint range of motion or painful joint motion
Elbow Bursitis • Tx: • RICE • Cessation of offending activity • Thermotherapy 48-72 hours following onset of symptoms • Consider compression/protective padding once activity can be resumed
Elbow Lateral Epicondylitis • Commonly referred to as “tennis elbow” due to its frequency of occurrence in tennis. • MOI: • Due to improper tennis backhand technique, improper tennis racket head or handle size, or excessive tennis backhand repetition.
Elbow Lateral Epicondylitis • S/S: • Pain, point tenderness over lateral epicondyle and extensor/suppinator muscle mass origin. • Possible inflammation over and near lateral epicondyle. • Pain with active wrist extension versus resistance, passive wrist flexion stretch, and varus stress.
Elbow Lateral Epicondylitis • TX: • RICE (ice massage appears to work well) • Cessation of offending activity • Thermotherapy 48-72 hours following onset of symptoms • Pain-free stretching • Gradual strengthening exercises • Consider selecting more appropriate size racket head or handle and or practice correct mechanics depending on etiology
Elbow Medial Epicondylitis • Commonly referred to as “little league elbow” due to its frequency of occurrence to adolescent baseball athletes. • MOI: • Due to improper throwing mechanics or excessive repetitive stress. • More common in adolescents due to the apohyseal plate of the medial epicondyle being open to allow for widening growth of the humerus at the distal end. • Resulting pulling force of the flexor/pronator muscles on the medial epicondyle results in traction apophysitis, or inflammation of the medial epicondylarapophysis due to traction forces.
Elbow Medial Epicondylitis • S/S: • Pain, point tenderness over medial epiconyle and flexor/pronator muscle mass origin. • Possible inflammation near medial epicondyle. • Pain with active wrist flexion versus resistance, passive wrist extension stretch and valgus stress.
Elbow Medial Epicondylitis • TX: • RICE • Cessation of offending activity • Thermotherapy 48-72 hours following onset of symptoms • Pain-free stretching • Gradual strengthening exercises • Consider practicing correct throwing mechanics to prevent re-injury
Criteria for advancing to phase II PHASE I: Immobilization/ Pain Managment Rehabilitation Method Pain Management: Splint/Cast Immobilization Ice Heat NSAIDS Limiting Atrophy: Isometrics Maintain Conditioning Stationary Cycle Lower Extremity Weight Training Sufficient Healing Time/Removal of Splint or Cast by Physician
Criteria for advancing to Phase III PHASE II:Range of Motion Rehabilitation Method Joint Flexibility Exercises: Active ROM Passive ROM Joint Mobilization Therapeutic Modalities: Thermotherapy Hydrotherapy Limiting Atrophy: Isometric contractions throughout the available pain-free areas of ROM Maintain Conditioning: Stationary Cycle Lower Extremity Weight Training 85-90% return of pre-injury ROM
Criteria for Advancing to Phase IV PHASE III: Basic Strength Rehabilitation Method Basic Elbow/Forearm Strengthening Exercises: Manual Resistance Rubber cord/tubing Light weight dumbbell Therapeutic Modalities: Thermotherapy pre-exercise Ice post-exercise 85-90% return of pre-injury muscular strength
Criteria for advancing to Phase V PHASE IV: Speed/Power/Endurance Rehabilitation Method Speed Exercises: Bouncy Ball Plyoback (light ball) Power Exercises: Upper extremity plyometrics Plyoback (heavy ball) Foam Roller Endurance Exercises: Rubber Tubing or light weight dumbbell repetitions to fatigue 85-90% return of pre-injury speed, power and endurance
Criteria For Advancing to Phase VI PHASE V:Sport Specific Exercise Rehabilitation Method Exercises that mimic movement in the injured athletes specific sport, (throwing, weight support, etc.) Exercises gradually progress from low to high intensity, resistance and speed Athlete demonstrates ability to perform sport-specific drills at full intensity without pain or post-exercise inflammation
Criteria for advancing to full clearance without restrictions PHASE VI: Return to Play Rehabilitation Method Gradual progression from limited participation with restrictions (i.e., no contact-limited contact-partial contact) to full participation with no restrictions Athlete demonstrates ability to participate in full practice without pain or evidence of post-exercise swelling
Terminology • Carpals: small bones of the hand • Metacarpals: long bones of the hand, between the carpal bones and the phalanges • Phalanges: bones of the fingers • Saddle joint: an articulation between concave and convex ends of bones
Terminology Anatomical snuffbox: a depression over the wrist that can be seen when the fingers are extended Avascular necrosis: tissue death due to lack of blood supply Boxer’s fracture: injury of the 5th metacarpal Colles’ fracture: fracture of the distal radius
Terminology Carpal tunnel: area on the anterior wrist where the median nerve and tendons cross the wrist and are enclosed by the transverse carpal ligament Paresthesia: tingling sensation or loss of normal sensation
Bones of the Hand & Wrist • Ulna • Radius • Carpals (8) • Metacarpals (5) • Phalanges (14) • Distal • Intermediate • Proximal http://www.sports-injury-info.com/hand-anatomy.html